Lumbar Stress Fractures in Cricket Players
Relevant Anatomy[edit | edit source]

The lumbar vertebrae is made up of 5 different bones L1 is the most superior and L5 the most inferior. These 5 vertebrae share most of the same features and have very similar function. All stress fractures in the lumbar spine occur at either L3 (12% of stress fractures), L4 (35% of stress fractures) or L5 (32% of stress fractures). The remaining percentages account for fractures in multiple locations (Alway et al, 2019).
There are three joints between each vertebra, two facet joints (also known as zygapophyseal joints) which are on either side and also a vertebral disc joint in the centre of the vertebrae. These joints do not allow for much movement as the lumbar structures are very stable.
Movement at the lumbar joints[edit | edit source]
Different joints in the lumbar spine allow for differing degrees of movement. All of the lumbar spine joints allow for most movement within the sagittal plane allowing for flexion and extension. L1 allows for around 12 degrees whereas L5 allows for around 17 degrees (these numbers change based on individual differences).
Lumbar stress fractures more frequently occur at the lower vertebrae this is because lumbar stress fractures occur as a result of extension related forces so the vertebrae that allow for more extension are more likely to be injured.

Stress fractures[edit | edit source]
Stress fractures are small cracks within a bone. For something to be defined as a stress fracture there must be a clear crack in the bone without it being a complete crack as that would be a different type of fracture(Astur et al., 2016).In the lumbar spine this crack can appear in two different locations. The pars interarticularis (77.2% of lumbar stress fractures) and the pedicle (22.8% of stress fractures) (Alway et al, 2019). A stress fracture at the pars interarticularis is more frequently referred to as a spondylolysis.
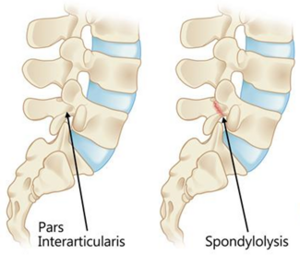
77.2% of lumbar stress fractures occur at the Pars Interarticularis, these fractures are also known as spondylolysis'
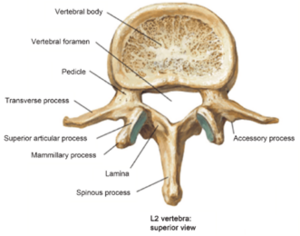
This is a typical lumbar vertebrae, note the pedicle labelled on the left of the image 22.8% of lumbar stress fractures occur here


Pathology [edit | edit source]
Stress fractures are overuse injuries. In the presence of repetitive loading and inadequate time for healing and recovery. The repetitive stress response leads to increased osteoclastic activity surpassing the rate of osteoblastic activity, this causes weakening of the bone making it susceptible to stress fracture. Over time the fracture develops. Fatigue in other structures around the vertebrae is a common cause of the stress fracture.
In healthy bone repair occurs thanks to osteoblastic activity. However, when the recovery period is insufficient for long periods of time the boney repair doesn’t happen and so the repetitive loading causes microfractures which develop into full stress fractures(Kiel and Kaiser, 2020).
Epidemiology[edit | edit source]
Stress fractures of the lumbar spine represent 15% of all missed playing time in cricket, and up to 67% of fast bowlers will sustain this injury during their career (Farhart et al., 2023). Furthermore, lumbar stress fracture result in the greatest time loss of any injury suffered in cricket due to the long recovery process as well as managing pain and function levels (Farhart et al., 2023). If not taken care of this can lead to a much more serious condition called spondylolisthesis where a vertebral body slips out of line causing radicular or mechanical pain usually due to nerve root compression.
Keylock et al. (2022) highlighted the increased vulnerability of adolescents to lumbar stress fractures, particularly when transitioning to higher-level teams. The escalation in bowling workload and intensity at senior levels, coupled with the relatively immature and less robust lumbar spine in late adolescence, predisposes players to these injuries. This vulnerability arises from large ground reaction forces and extreme multiplanar trunk movements which impose significant shear and compressive stress on the lumbar spine as well as the full ossification of the lumbar spine not occurring until the age of 25. A study examining bowling workload in English county cricketers revealed that bowling more than 234 deliveries in a 7-day period significantly increases the risk of lumbar stress fractures compared to bowling fewer than 197 deliveries (Alway et al., 2019). Furthermore, Orchard et al in 2010 found that pace bowlers with a previous history of lumbar stress fractures are more at risk of lower limb muscle strains. This is because of bony hypertrophy associated with stress fracture healing may lead to lumbar nerve root impingement, making lower limb muscle strains more likely to occur especially in the calf. Implementing rating of perceived exertion (RPE) measures for self-management as well as implementing guidelines for fast bowling workload could be beneficial for reducing the incidence of these lumbar stress fractures in athletes under the age of 25.
Biomechanical Underpinnings The fast-bowling action is a complex sequence of movements that places significant stress on the lumbar spine. The action commences during the delivery stride prior to ball release, with the first key event being back foot contact (BFC) when the bowler's back foot impacts the ground (Bartlett, 1996). This is followed by front-foot contact (FFC) after ball release. Fast bowling actions can be broadly categorised into one of four types: front-on, side-on, semi-open, and mixed (Thiagarajan et al., 2015). This categorisation is determined according to the alignment of the shoulders at BFC and the amount of shoulder counter-rotation during the delivery stride (Portus et al., 2004).
[Image 1: Illustration of the four bowling action types]
The Mixed Bowling Action Research by Cook et al. (2015) identifies a strong correlation between the "mixed action" bowling style and an increased prevalence of lumbar stress fractures. This action is characterised by a significant angular disparity (>40 degrees) between the hips and shoulders, as well as excessive counter-rotation of the torso. This action leads to several detrimental effects: Excessive extension and rotation, placing undue stress on the pars interarticularis, a vulnerable region of the vertebrae. Repetitive lumbar hyperextension, with the bowler's front foot landing while the torso is in a hyperextended position. This places high loads on the posterior elements of the lumbar vertebrae, particularly the pars interarticularis, leading to potential microfractures over time.
Rotational forces, as the bowling action involves a forceful rotation of the torso to generate pace. This rotation, combined with hyperextension, creates a complex stress pattern on the spine, further increasing the risk of fractures. Lateral flexion, where some bowlers, particularly younger athletes, may exhibit uncontrolled lateral flexion of the spine during the delivery stride. This uneven loading on the vertebrae increases the risk of injury, as evidenced by Hibbert et al. (2018). Their research introduced the "crunch factor," which considers both lateral flexion and rotational velocity of the lumbar spine. A higher "crunch factor" has been linked to a greater risk of stress fractures on the side opposite the bowling arm.
[Image 2: Illustration of the mixed bowling action and associated forces]
Ground Reaction Forces and Altered Stress Distribution During the fast bowling delivery stride, peak ground reaction forces can reach up to nine times the bowler's body weight (Linthorne et al., 2015). These substantial forces are transmitted through the body, impacting the lumbar facet joints. If the bowler's front foot lands while the spine is in a combined state of rotation, extension, and lateral flexion, the stress distribution on the spine is disrupted (Linthorne et al., 2015). This abnormal loading places excessive strain on the pars interarticularis, as the forces are not absorbed efficiently, increasing the fracture risk.
[Image 3: Diagram showing ground reaction forces and stress distribution]
Bowling Workload and Fatigue-Induced Technique Breakdown First-class bowlers can deliver a significant number of balls (300-500) per week during a season (Linthorne et al., 2015). Inadequate workload management can have detrimental consequences. Research by Gabbett et al. (2011) suggests that bowling too many overs in a single session can lead to fatigue, causing technique to deteriorate. This can manifest as increased counter-rotation, further stressing the lumbar spine. Additionally, a study by Cumming et al. (2015) demonstrated that junior fast bowlers with less than 3.5 days of recovery between bowling sessions were three times more likely to sustain injuries, including lumbar stress fractures.
Risk Factors Beyond Biomechanics While biomechanics play a central role, several other factors contribute to a fast bowler's susceptibility to lumbar stress fractures. Improper bowling mechanics, such as excessive shoulder counter-rotation in adolescents or uncontrolled trunk rotation in adults, can place additional stress on the lumbar spine. Fast bowlers with high delivery volumes, especially those experiencing rapid increases in workload (e.g., transitioning from junior to senior cricket), are more likely to develop stress fractures due to insufficient time for bone adaptation.
Adolescent bowlers (aged 15-18) are particularly vulnerable due to their growing skeletons. Their bones are not yet fully mature and can be less tolerant of the repetitive stress of fast bowling. A weak core or imbalances between core muscle groups can lead to uneven stress distribution on the spine, compromising its stability and increasing the risk of fractures. Bowlers with pre-existing lower back issues are also at greater risk. Furthermore, bowlers with larger body sizes may experience higher loads on their lumbar spine during bowling, and inadequate levels of vitamin D and bone calcium can compromise bone health and increase susceptibility to stress fractures.
Lumbar stress fractures are a significant concern for fast bowlers in cricket, with the biomechanics of the bowling action and various risk factors contributing to their development. By understanding the underlying mechanisms, such as the impact of mixed bowling actions, ground reaction forces, and workload management, teams can implement targeted preventive measures. These measures include technical coaching, workload monitoring, strength and conditioning programs, and early screening and intervention. Through a comprehensive approach, cricket teams can mitigate the risk of these debilitating injuries, ensuring the longevity and success of their fast bowling talents.
Diagnosis[edit | edit source]
When assessing a patient with a lumbar stress fracture, typical clinical findings include a hyper lordotic posture and low back pain exacerbated by lumbar spine extension. Additional common symptoms may include swelling, pain, which can also radiate into the lower legs, with heightened symptoms during activity and alleviation at rest. Neurological assessment becomes necessary if patients experience numbness or tingling, although this occurrence is more prevalent in athletes with spondylolisthesis. Assessing patients with lumbar stress fractures can be challenging, as many cases are asymptomatic. However, bone marrow edema levels can be evaluated as an indicator of early response to stress fractures in the lumbar spine as it has been proven that these levels increase as the first response even without a visible fracture line on a MRI scan (Nakamae et al., 2021).
Roland-Morris questionnaire is a tool that is used to assess disability levels concerning low back pain. This would be relevant if the athletes symptoms are causing mild-severe disability due to pain levels. The score ranges from 0 (no disability) to 24 (max. disability) depending on the questionnaire used (Roland and Morris, 1983). This tool can also be used to measure progression as you can get the patient to fill this out before and after treatment to see how much their disability score has improved.
CT, SPECT and MRI scans have all been shown to be an effective tool in identifying lumbar stress fractures. However, one factor to consider is the amount of radiation exposure for adolescents as previously mentioned they are at a higher risk to these fractures.
Management/Interventions[edit | edit source]
The aim of management strategies in athletes presenting with lumbar stress fractures is to achieve bony union, avoid reoccurrence and return to sport (1). Cricket players’ ability to return to sport following lumbar stress fractures, consist of two important aspects: time of return and quality of performance following return (2). Management options include surgical and conservative interventions. It is essential to treat each athlete individually, considering their functional limitations, symptoms, level of participation, personal goals and any psychosocial factors that need consideration (3).
Surgical Management[edit | edit source]
Amongst cricketer’s, surgery should only be considered if conservative treatment has previously failed or chronic pars defects are present and show no potential signs of healing (10). This method should only occur if truly necessary and is stated surgery may be considered if 6 months of attempted conservative management is unsuccessful (10). Pars interarticularis repair is recommended with excellent results in returning to bowling being demonstrated in multiple studies (6)(8). Fusion surgery is another surgical modality and should be avoided especially in the younger age groups due to association to reduced spinal flexibility and degeneration (9)
Conservative Management[edit | edit source]
Conservative treatment should commence if an acute stress fracture is diagnosed and demonstrates potential to heal (9). A Systematic Review comparing return to sport time between conservative and surgical treatment showed averages of around 4.9 and 6.4 months respectively (5). Returning to their pre injury level was found to occur in 81% post-surgery of athletes as opposed to 89% following conservative treatment (5).
Sport Cessation[edit | edit source]
Treatment should begin with complete cessation of sporting and impact activities for 12 weeks followed by bracing upon return (9). Studies showed significantly lower functional outcomes and sport performance are present in athletes choosing to continue sport with a brace compared to players simply resting from sport for 3 months (10).
Bracing[edit | edit source]
A study (4) comparing patients with and without bracing found no significant advantage of brace us in achieving bony union. Although the sample size was small, it appears bracing’s primary function involves the limitation in Range of Motion as opposed to stabilising the fracture (3). Studies suggests that compliance with the bracing significantly impacts clinical outcomes and return to play with the specific brace being less important (10).
Patient Re-education[edit | edit source]
Another important part of the rehabilitation involves patient re-education surrounding their bowling technique to aim to lower the stresses placed on the lumbar region, without decreasing performance (6). Fast bowlers that are classified as having a ‘mixed bowling technique’ are at greater risk due to the shoulders rotating in relation to the pelvis which remains front on (6). These bowlers have been shown to be less likely to respond to conservative management, highlighted by a study of 7 of 8 cricketers that required surgery bowled with a ‘Mixed’ technique (6). Since lumbar stress fractures occur more predominantly in younger athletes, ensuring alteration in their bowling technique is necessary (6). Younger athletes are significantly better at responding to these proposed adaptations highlighting the importance of early intervention from coaches or performance analysts (6). Reassurance that their bowling performance won’t decrease by imposing these changes is essential, with no changes to bowling speed being found (7) Balancing the amount of bowling junior players perform whilst still providing them with the necessary experience to improve should also be considered (6).
Psychosocial Factors[edit | edit source]
Psychosocial factors such as fear avoidance and emotional distress should also be addressed. Along with physical factors, all athletes are susceptible to experiencing anxiety, lowered self-esteem, isolation and depression following injury and during rehabilitation (11). Therefore, it is essential to provide an excellent social support to all patients, through establishing a positive relationship and demonstrating excellent communication to direct each patient to seek out the support they require (11).
Lumbar Stress Fracture Rehabilitation Protocol[edit | edit source]
Rehabilitation should then be implemented with primary focuses on anti-lordotic exercises, abdominal strengthening and hamstring stretching (9). There is lacking evidence on specific spondylolysis protocols among cricket players, but a systematic physical rehabilitation program is likely most effective (9). The phases and goals of rehabilitation below, have been designed using protocols drawn from the literature (9)(11):
Phase 1: Rest and Protection (0-12 weeks)
This involves complete rest from any aggravating activities. It is important to allow the lumbar region to have adequate healing time. Mobility should be maintained ensuring symptoms don’t worsen.
- Patient Education on fear of movement and encourage ADLs
- Hip Flexor and Hamstring Mobility
- Core activation (No Active or Passive Spinal Extension)
- Pelvic floor control exercises
Phase 2: Trunk Stabilisation + ROM
Activity is limited to pelvic control and core stability exercises which both aim to correct postural alignment issues and decrease the load placed on the pars interarticularis especially during extension exercises. Introduction of spinal extension and rotation movements.
- Dynamic core, glute and spinal movements (Limit Spinal Extension)
- Static Trunk Strengthening
- Continue and Progress ROM
- Proprioceptive Exercise
- Bulleted list item
Phase 3: Strength + Sport Specific
This phase involves the introduction of dynamic trunk exercises. Lumbar ROM should increase with more movements in Spinal Extension being permitted as long as they remain pain free. Non-weight bearing (NWB) cardiovascular training should be introduced such as Swimming or Cycling. Cricket specific drills should also be implemented focusing on coordination, catching and throwing to focus on motor skill development.
- Dynamic Trunk Strengthening
- Introduce Spinal Extension Movements
- Introduce Cardiovascular Training (NWB)
- Cricket Specific Drills
Phase 4: Return to Play
The final phase is return to play which should begin if the previous phase is achieved in a pain free manner. Before returning to sport all cricket players should ensure to be pain free in all functional activities as well as restoring full ROM, baseline strength and cardiovascular fitness (3).
- Advanced Strengthening- Trunk + Lower Limb
- Plyometrics
- Agility, FWB Cardiovascular Training
- Bowling Technique Alterations
References[edit | edit source]
Alway, P., Brooke-Wavell, K., Langley, B., King, M. and Peirce, N. (2019). Incidence and prevalence of lumbar stress fracture in English County Cricket fast bowlers, association with bowling workload and seasonal variation. BMJ Open Sport & Exercise Medicine, [online] 5(1), p.e000529. doi:https://doi.org/10.1136/bmjsem-2019-000529.
Astur, D.C., Zanatta, F., Arliani, G.G., Moraes, E.R., Pochini, A. de C. and Ejnisman, B. (2016). Stress fractures: definition, diagnosis and treatment. Revista Brasileira de Ortopedia (English Edition), [online] 51(1), pp.3–10. doi:https://doi.org/10.1016/j.rboe.2015.12.008.
Farhart, P., Beakley, D., Diwan, A., Duffield, R., Rodriguez, E.P., Chamoli, U. and Watsford, M., 2023. Intrinsic variables associated with low back pain and lumbar spine injury in fast bowlers in cricket: a systematic review. BMC Sports Science, Medicine and Rehabilitation, 15(1), p.114.
Keylock, L., Alway, P., Felton, P., McCaig, S., Brooke-Wavell, K., King, M. and Peirce, N., 2022. Lumbar bone stress injuries and risk factors in adolescent cricket fast bowlers. Journal of Sports Sciences, 40(12), pp.1336-1342.
Kiel, J. and Kaiser, K. (2020). Stress Reaction and Fractures. [online] PubMed. Available at: https://www.ncbi.nlm.nih.gov/books/NBK507835/ [Accessed 18 Mar. 2024].
Nakamae, T., Kamei, N., Tamura, T., Kanda, T., Nakanishi, K. and Adachi, N., 2021. Quantitative assessment of bone marrow edema in adolescent athletes with lumbar spondylolysis using contrast ratio on magnetic resonance imaging. Asian Spine Journal, 15(5), p.682. Sassack, B. and Carrier, J.D. (2020). Anatomy, Back, Lumbar Spine. [online] PubMed. Available at: https://www.ncbi.nlm.nih.gov/books/NBK557616/ [Accessed 18 Mar. 2024].
Orchard, J., Farhart, P., Kountouris, A., James, T. and Portus, M., 2010. Pace bowlers in cricket with history of lumbar stress fracture have increased risk of lower limb muscle strains, particularly calf strains. Open Access Journal of Sports Medicine, pp.177-182. Roland, M. and Morris, R., 1983. A study of the natural history of back pain: part I: development of a reliable and sensitive measure of disability in low-back pain. spine, 8(2), pp.141-144.
Schouten, R., Shackel, D. and Inglis, G., 2021. Surgical repair of lumbar stress fractures in professional cricketers. Journal of Spine Surgery, 7(3), p.385.

