Basal Ganglia
Introduction to the Basal Ganglia[edit | edit source]

The basal ganglia is not a single structure in the brain but rather are a group of subcortical nuclei and other associated structures, located at the base of the forebrain.[1]
They are primarily involved in motor control and motor initiation[2], as well as motor learning, executive functions and emotional behaviours. The basal ganglia also play an important role in reward and reinforcement, addictive behaviours and habit formation.[3]
Basal ganglia network dysfunction can lead to various movement disorders,[3] such as Parkinson's and Huntington disease.
Structure of the Basal Ganglia[edit | edit source]
The basal ganglia is made up of multiple separate structures that link together in several different ways. The interconnected pathways are what define the function of the basal ganglia. Below is a photo gallery which shows different views of the basal ganglia to include its various structures and neural networks.

Basal ganglia nuclei

Corpus striatum of the basal ganglia
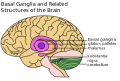
Basal ganglia structures

Basal ganglia nuclei in relation to other subcortical structures.




Corpus Striatum[edit | edit source]
Corpus Striatum is the largest component of the basal ganglia, it is a heterogeneous structure with a volume of around 10 cm3. It receives afferent inputs from various cortical and subcortical structures and sends outputs to different basal ganglia nuclei.[3]
There are two main divisions in the corpus striatum:
- Dorsal Striatum (DS): mostly involved in the control of conscious motor movements and executive functions.
- Caudate nucleus: is a paired subcortical structure and is involved in many "higher" neurological functions such as (1) movement execution, (2) learning, (3) memory, (4) reward and motivation, (5) emotion, and (6) "romantic interactions"[4]
- Ventral Striatum: involved in the limbic functions of reward and aversion. It is made up of the nucleus accumbens and the olfactory tubercle.[2]
- Nucleus accumbens in the neural interface between "motivation and action" or the "limbic-motor interface" It is involved in a wide range of goal-directed behaviors including (1) feeding, (2) sexual, (3) reward, (4) stress-related, and (5) drug self-administration[5]
- Olfactory tubercle is thought to be involved in odor-guided motivated and eating behaviours.[6] It likely works in tandem with the nucleus accumbens.
Lenticular Nuclei[edit | edit source]
- Putamen: communicates with many different regions of the cerebral cortex and forms multiple connections within the basal ganglia. It is involved in (1) learning and motor control, (2) speech articulation, (3) language functions, (4) reward, (5) cognitive functioning, and (6) addiction. The putamen also plays a role in modulating sensory and motor aspects of pain.[7]
- Globus Pallidus which can be further divided into two parts: globus pallidus externus, and internus. [8] The primary role of the globus pallius is controlling conscious and proprioceptive movements.[9]
Subthalamic Nucleus[edit | edit source]
Subthalamic Nucleus (STN): a lens-shaped cell group that makes up a large part of the subthalamus.[10] It has neural projections into the globus pallidus and assists with movement regulation. Specifically, the subthalmic nucleus plays a critical role in the prevention of unwanted movements. For example, a lesion of the subthalamic nucleus can result in hemiballismus (please see below for more details on this disorder).[11]
Substantia Nigra[edit | edit source]
Substantia Nigra, means "black substance" in Latin. The substantia nigra is located in the midbrain but is considered part of the basal ganglia.[12] The substania nigra is critical in modulating motor movement and reward functions as part of the greater basal ganglia circuitry. Of great clinical significance are connections between the substantia nigra and the putamen. Damage to this connection has been linked to the motor deficits seen in persons with Parkinson's. [13]
The two optional videos below provide further information on the structure and function of the basal ganglia:
Function of the Basal Ganglia[edit | edit source]
The classical basal ganglia model suggested that "information flows through the basal ganglia back to the cortex through two pathways with opposing effects for the proper execution of movement."[16] In this "loop", cortical input is sent to the basal ganglia, where it is modified and then sent back to the cortex. As a result of this feedback, motor activity is either facilitated or inhibited.[16]
This model has been reviewed and updated. It is now believed that the basal ganglia have "multiple parallel loops and re-entering circuits whereby motor, associative, and limbic territories are engaged mainly in the control of movement, behaviour, and emotions."[16]
The following image illustrates various excitatory and inhibitory pathways from the basal ganglia to the cortex.[3]

Associated Conditions[edit | edit source]
Dysfunction of the basal ganglia is associated with specific movement disorders, and can cause issues such as (1) tremor, (2) involuntary muscle movements, (3) abnormal increase in tone, (4) difficulty initiating movements, and (5) abnormal posture. The following sections discuss movement disorders associated with basal ganglia dysfunction.[2]
Parkinson's[edit | edit source]
Parkinson's is the second most common neurodegenerative disorder. Its aetiology is multifactorial, with both genetic and environmental risk factors identified.[17] Parkinson's is characterised "by the progressive loss of dopaminergic neurons and the formation of Lewy bodies in the affected brain areas".[18] Because of the degeneration of dopaminergic neurons, there is less dopamine available in the substantia nigra and striatum, which causes various clinical signs of Parkinson's, such as:[18]
- tremor
- postural instability
- bradykinesia or slow movement
- rigidity or stiffness
- decreased coordination
- shuffling gait
Huntington's Disease[edit | edit source]
Huntington's disease[19] is a progressive, inherited neurodegenerative disease. It is associated with neuropsychiatric symptoms, movement disorders (usually chorea) and cognitive impairment / dementia.[20][21] Huntington's disease occurs in individuals with a CAG expansion in the huntingtin gene.[20] There is neurodegeneration in many parts of the brain, the striatum[20] and cortex are particularly affected.[22] Symptoms usually start in individuals aged between 30-50 years. A key motor symptom is chorea (i.e. "brief, involuntary movements that generally affect the trunk, face, and arms"[22]). Chorea affects voluntary movements, ultimately affecting walking, speaking and swallowing.[22]
Cognitive impairments include:[22]
- decreased executive function (difficulty with attention, concentration, multi-tasking, decision making)
- depression
- loss of memory
- decreased insight
The most common psychiatric conditions are:[22]
- depression
- irritability
- increased impulsivity
Hemiballism[edit | edit source]
Hemiballism (from the verb “to throw” in Greek) is a rare movement disorder that causes "high amplitude movement of an entire limb or limbs on one side of the body."[23] Hemiballism can be caused by several conditions, but acute cases are often associated with focal lesions in the contralateral basal ganglia and subthalamic nucleus lesion.[23] Individuals with hemiballism tend to have a good prognosis.[23]
Tourette Syndrome[edit | edit source]
Tourette syndrome is a persistent neurodevelopmental condition associated with motor and phonic tics.[24] While its pathophysiology is not fully understood, tics may be due to "inhibitory dysfunction within the sensorimotor cortico-basal ganglia network".[24] Tourette syndrome can significantly impact quality of life, and treatment options are expanding.[24]
References[edit | edit source]
- ↑ Yanagisawa N. Functions and dysfunctions of the basal ganglia in humans. Proc Jpn Acad Ser B Phys Biol Sci. 2018;94(7):275-304.
- ↑ 2.0 2.1 2.2 Young CB, Sonne J. Neuroanatomy, basal ganglia. InStatPearls [Internet] 2018 Dec 28. StatPearls Publishing.
- ↑ 3.0 3.1 3.2 3.3 Lanciego JL, Luquin N, Obeso JA. Functional neuroanatomy of the basal ganglia. Cold Spring Harbor perspectives in medicine. 2012 Dec 1;2(12):a009621.
- ↑ Driscoll; M, Bollu P, Tadi P. Neuroanatomy, Nucleus Caudate [Internet]. 24 July 2024 [cited 01 July 2024]. Available from:https://www.ncbi.nlm.nih.gov/books/NBK557407/
- ↑ Fernández-Espejo E. How does the nucleus accumbens function? [Internet]. 2000 May;30(9):845-9.[cited 01 July 2024]. Available from: https://pubmed.ncbi.nlm.nih.gov/10870199/
- ↑ Murata K. Hypothetical Roles of the Olfactory Tubercle in Odor-Guided Eating Behavior [Internet]. Front Neural Circuits. 2020; 14: 577880..[cited 01 July 2024]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7686465/
- ↑ Ghandili M, Munakomi S. Neuroanatomy, Putamen [Internet]. 30 January 2023 [cited 01 July 2024]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK542170/
- ↑ Javed N, Cascella M. Neuroanatomy, Globus Pallidus. [Updated 2023 Feb 20]. In: StatPearls [Internet].
- ↑ Javed N, Cascella M. Neuroanatomy, Globus Pallidus [Internet]. 20 February 2023 [cited 01 July 2024]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557755/
- ↑ Basinger H, Joseph J. Neuroanatomy, Subthalamic Nucleus. [Updated 2022 Oct 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559002/
- ↑ Basinger H, Joseph J. Neuroanatomy, Subthalamic Nucleus [Internet]. 31 October 2022 [cited 01 July 2024]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559002/
- ↑ Jacobs LK, Sapers BL. Neurological Disease. InPerioperative Medicine 2011 (pp. 343-359). Springer, London.
- ↑ Sonne J, Reddy V, Beato MR. Neuroanatomy, Substantia Nigra [Internet]. 24 October 2022 [cited 01 July 2024]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536995/
- ↑ Neuroscientifically Challenged Basal ganglia . Available from: https://www.youtube.com/watch?v=OD2KPSGZ1No [last accessed 14/01/2020]
- ↑ Armando Hasudungan. The Basal Ganglia Clinical Anatomy. Available from: https://www.youtube.com/watch?v=mNc-6q6YAAw [last accessed 05/01/2024]
- ↑ 16.0 16.1 16.2 Lanciego JL, Luquin N, Obeso JA. Functional neuroanatomy of the basal ganglia. Cold Spring Harbor perspectives in medicine. 2012 Dec 1;2(12):a009621.
- ↑ Ben-Shlomo Y, Darweesh S, Llibre-Guerra J, Marras C, San Luciano M, Tanner C. The epidemiology of Parkinson's disease. The Lancet. 2024;403(10423):283-92.
- ↑ 18.0 18.1 Zhou, ZD, Yi LX, Wang DQ, Lim TM, Tan EK. Role of dopamine in the pathophysiology of Parkinson’s disease. Transl Neurodegener. 2023;12(44).
- ↑ Matz OC, Spocter M. The Effect of Huntington's Disease on the Basal Nuclei: A Review. Cureus. 2022;14(4):e24473.
- ↑ 20.0 20.1 20.2 Stoker TB, Mason SL, Greenland JC, Holden ST, Santini H, Barker RA. Huntington's disease: diagnosis and management. Pract Neurol. 2022 Feb;22(1):32-41.
- ↑ Medina A, Mahjoub Y, Shaver L, Pringsheim T. Prevalence and incidence of Huntington's disease: an updated systematic review and meta-analysis. Mov Disord. 2022 Dec;37(12):2327-35.
- ↑ 22.0 22.1 22.2 22.3 22.4 Kim A, Lalonde K, Truesdell A, Gomes Welter P, Brocardo PS, Rosenstock TR, Gil-Mohapel J. New avenues for the treatment of Huntington's disease. Int J Mol Sci. 2021 Aug 4;22(16):8363.
- ↑ 23.0 23.1 23.2 Hawley JS, Weiner WJ. Hemiballismus: current concepts and review. Parkinsonism Relat Disord. 2012 Feb;18(2):125-9.
- ↑ 24.0 24.1 24.2 Johnson KA, Worbe Y, Foote KD, Butson CR, Gunduz A, Okun MS. Tourette syndrome: clinical features, pathophysiology, and treatment. Lancet Neurol. 2023 Feb;22(2):147-58.

