Fitness and Low Back Pain: Difference between revisions
George Smith (talk | contribs) No edit summary |
George Smith (talk | contribs) No edit summary |
||
| Line 105: | Line 105: | ||
== <br><br><br>Strength and Low Back pain == | == <br><br><br>Strength and Low Back pain == | ||
<br>Muscle strength is the contractile force a muscle is able to produce. <br> The large muscles of the back (See anatomy section) are often thought of as synomous with back strength. ( <ref name="Lee et al 2012">Lee HJ, Lim WH, Park JW, Kwon BS, Ryu KH, Lee JH, Park YG. The Relationship between Cross Sectional Area and Strength of Back Muscles in Patients with Chronic Low Back Pain. Ann Rehabil Med. 2012</ref> ) It is a commonly held belief that having 'strong' back muscles support the back and prevent back pain however there is conjecture in the literature surrounding this theory. <br> <br> Many common exercises such as prone extensions, dead lifts and low-rows are thought to strengthen the back muscles and 'stabalise' the spine or prevent injury. Muscle strengthening exercises form part of the NICE treatment guidelines for Early management of persistent non-specific low back pain ( <ref name="NICE 2009">NICE : CG88 Low back pain: Early management of persistent non-specific low back pain 2009</ref> ). <br> <br> [[Image:Back pain strength.jpg|580x200px]]<br> | <br>Muscle strength is the contractile force a muscle is able to produce. <br> The large muscles of the back (See anatomy section) are often thought of as synomous with back strength. ( <ref name="Lee et al 2012">Lee HJ, Lim WH, Park JW, Kwon BS, Ryu KH, Lee JH, Park YG. The Relationship between Cross Sectional Area and Strength of Back Muscles in Patients with Chronic Low Back Pain. Ann Rehabil Med. 2012</ref> ) It is a commonly held belief that having 'strong' back muscles will support the back and prevent back pain however there is conjecture in the literature surrounding this theory. <br> <br> Many common exercises such as prone extensions, dead lifts and low-rows are thought to strengthen the back muscles and 'stabalise' the spine or prevent injury. Muscle strengthening exercises form part of the NICE treatment guidelines for Early management of persistent non-specific low back pain ( <ref name="NICE 2009">NICE : CG88 Low back pain: Early management of persistent non-specific low back pain 2009</ref> ). | ||
<br> <br> [[Image:Back pain strength.jpg|580x200px]]<br> | |||
<br> | <br> | ||
Revision as of 19:42, 19 January 2014
</div>
Introduction
[edit | edit source]
The aim of this page is to present an overview of the relationship between Fitness and Low Back Pain and to establish to what extent being fit or having a high level of fitness affects your risk of devloping back pain or prevents future episodes.
A brief introduction to back pain is provided with links to further reading on the topic. Relevant anatomy is dicussed with regards to structural sources of pain.
The various different aspects of physical fitness are discussed and their relationship with back pain making reference to best evidence to summarise into clinically significant conlusions.
Defining Low Back Pain (LBP) [edit | edit source]
• Low back pain is an umbrella of conditions with 80% of adults estimated to experience LBP at some point during their life ( [1] )
• Male and female individuals are affected equally ( [2] ).
• Low back pain encompasses and pain between the bottom of the ribs and the buttock crease.
• Common subdivisions of LBP are acute, sub-acute or chronic/persistent and specific or non-specific
• The three most common diagnostic methods are (in no particular order) Maitland, McKenzie and a Movement based assessment.
• Low back pain guidelines
Specific vs Non-specific[edit | edit source]
Specific low back pain refers to the diagnosis of a specific cause/structure such as a malignancy, fracture, or disk bulge etc. Specific low back pain should be identified with appropriate triage and the appropriate investigations undertaking. (Red Flags in spinal cases).
Non-specific low back pain is much more common and evidence suggests it accounts for approx. 95% of back pain, ( [3] )

Acute/Sub-acute and Chronic Low Back Pain [edit | edit source]
Alongside specific and non-specific, back pain is also defined by its duration. (See figure 1)
Figure 1: Time scales in non-specific low back pain for first episode: [5]

See also : Chronic Low Back Pain
Chronic Low Back Pain is a complex topic in itself and beyond the scope of this page however the link above has more information.
Relevant anatomy to fitness and LBP.[edit | edit source]
Overview [edit | edit source]
As you can see from the diagram there are several sections of the spine; cervical, thoracic, lumbar and sacral.

The majority of Lower back pain (LBP) is related to issues originating in the lumbosacral region.
The lumbar spine consists of 5 segmental vertebrae (L1-L5) each separated by an intervertebral disc. The sacrum is also made of 5 vertebras but these fuse together starting at 16 and are completely fused by 34.Although it is widely thought that in lower back pain cases it isn’t possible to differentiate the causes, this will explain the various relevant anatomy that is commonly thought to lead to LBP.
Arthrogenic structures [edit | edit source]
The main synovial joint between each vertebrae is the facet joint (zygapophyseal joint), this is a saddle joint, between the upper segment’s inferior articular facet and the lower segment’s superior articular facet. These are differently shaped to the Thoracic and cervical facets, as lumbar facets run side by side rather than on top of each other and this is why the lumbar spine has a more prominent role in flexing and extending but very limited rotational and side flexion range.

This joint can often be a major cause of LBP, there is evidence showing that the facet joint pain can be responsible for up to 27% of cases in the lumbar spine. The facet joint pain can be caused by several issues, the first being arthiritic changes that just occur from being used so much, this normally present in the elderly population, a biomechanical issue can often cause the facet joints to be irritated this often linked to variances in the musculature. The lumbar spine also has a number of ligament structures that can be relevant in relation to LBP. Running along the spinous process’ is the Supraspinous ligament and between each process is the interspinous ligament, there is also a anterior longitudinal ligament and posterior longitudinal ligament that runs down either side of the vertebral bodies (the posterior longitudinal ligament is one of the structures found in the vertebral canal.)
There is also the ligament flava which runs between the laminae of adjacent vertebrae, hypertrophy of this ligament (often associated with zygapophyseal joint arthiritis) can lead to spinal stenosis.
Ligaments sprains can be the cause of LBP as people can over stretch or over load the spine due to occupational hazards, athletic demands or just any awkward lifting and this has been shown to lead to LBP. However it is not always due to sprains that heavy lifting could cause LBP
Intervertebral Disc [edit | edit source]
The intervertebral disc is made up of the Annulus fibrosis and the Nucleus Pulposus.
The annulus fibrosis is the outer ring of collagen fibres that form protective layer around the nucleus pulposus, which fills the inside of the disc and is mostly responsible for absorbing compressive forces.
Following on from the last section, heavy lifting can lead to LBP by causing a disc prolapse or bulge. This is when there are tears or trauma to the annulus fibrosis which can result in the Nucleus pulposus bulging or even protruding out of the annulus fibrosis, this can cause compression of the spinal chord or nerve roots leading to often sciatic pain or other neuro related pain issues. http://www.physio-pedia.com/Disc_HerniationThe IV disc can also degenerate, this often starts with the loss of fluid from the disc, which can cause the facet joints and whole vertebras to come closer together leading to increase wear and loading in those joints due to the reduction in shock absorption. For further info-
http://www.physio-pedia.com/Degenerative_Disc_Disease
Muscles[edit | edit source]
When talking about the muscles that help stabilise the lumbar spine people often talk about the “core”. The “core” is comprised of several groups of muscles including the transversus abdominus, multifidus, diaphragm and pelvic floor muscles. The multifidi is a bilateral muscle and originates from the posterior sacral surface, PSIS and posterior sacroiliac ligament as well as each transverse process of the vertebrae below the segment it inserts into. It inserts into the spinous process at the vertebrae above.
Advances in the understanding of the biomechanics of LBP have highlighted the importance of muscular stabilization of the "neutral zone" range of motion in the lower back. Multifidus muscles in the lumbar spine are important stabilizers of this neutral zone, and dysfunction in these muscles is strongly associated with LBP.
(http://www.ncbi.nlm.nih.gov/pubmed/20193941)

The pattern of multifidus muscle atrophy in chronic LBP patients is localized rather than generalized. Furthermore, between side asymmetry may be seen in chronic LBP patients presenting with a unilateral pain distribution.
(http://www.ncbi.nlm.nih.gov/pubmed/17070721)
The transverse abdominus (TvA) is the deepest of the abdominal muscles and is also a stabilizer of the spine. It has been found to be in a weakened state in those who have chronic back pain or problems. Its normal action along with the action of the the lumbar multifidus muscles function together to form a deep internal corset that acts to stabilize the spine during movement. This pattern of protection is disrupted in patients with low back pain.
It is uncertain why these muscles become dysfunctional after a low back injury, but specific exercises focusing on the contraction of these two muscles together will improve the protective stabilizing ability of the spinal muscles, reduce pain intensity, and improve activities of daily living as well as improve body awareness and posture.
Fitness [edit | edit source]
Physical fitness is a set of attributes that people have or achieve. Being physically fit has been defined as:- the ability to carry out daily tasks with vigour and alertness, without undue fatigue and with ample energy to enjoy leisure-time pursuits and meet unforeseen emergencies[6]
In accordance with Hales in 2010, these are the five components of physical fitness and the Gold Standards for measuring each of these aspects:-
1) Cardiorespiratory Endurance - VO2 max per Kg of body mass [7]
2) Muscular Endurance - Currently no Gold Standard measurment for muscular endurance
3) Muscular Strength - Isokinetic Dynamometry [8]
4) Body Composition:- The current Gold Standard is a Four-Compartment model of measurements most commonly consisting of Mass, Total Body Volume, Total Body Water and Bone Mineral Content. There are however other potential methods such as Dual-energy Xray Absorptiometry (DEXA) and Air-Displacement Plethsymology which are being trialled to measure body composition [9]
5) Flexibility - Optical Gold Standards such as the Vicon Motion Tracking System[10]
1) 3) 5)

Cardiorespiratory Endurance -[edit | edit source]
Cardiovascular Endurance is the ability of the circulatory and respiratory systems to supply fuel during sustained physical activity and eliminate fatigue products after supplying fuel. The pain relieving mechanics of aerobic exercise on lower back pain are not clear, since the intensity of the muscular contractions are not intense enough to promote muscular hypertrophy.
Cardiovascular (CV) fitness theoretically has many different influences on prevention of lower back pain. Cardiovascular fitness may help prevent any unfavourable adaptations to the body associated with neuromuscular health, muscular endurance, muscular strength and general loading through the lumbar spine.
The majority of these tend to be indirect effects as the association between cardiovascular fitness and LBP is not as discernible as that seen with muscular weakness, reduced flexibility and reduced muscular endurance.
However a more direct link to why high CV fitness can prevent lower back pain is that due to the avascular nature of the intervertebral discs they rely on osmosis for transport of nutrients and the removal of waste products. The improved efficiency in circulation that directly stems from good CV fitness, will facilitate the osmosis required to maintain disc hydration therefore delaying the process of disc degeneration and reducing the risk of LBP. (Plowman, 1992)
Smoking has also been shown to increase the likelihood of LBP. The causality of which can partially be explained by the physiological effects that smoking has on the CV system. The decreased arterial oxygen to the paraspinal muscles of the lower back will lead to muscle fatigue and increase the use of the lactic acid system, therefore lactic may build up and stimulate the pain sensors in the area, also as mentioned in Muscular endurance, the muscular fatigue increases the likelihood of low back pain too. (power,2001)
Muscular Endurance [edit | edit source]
Muscular Endurance is the ability of the muscle to exert a submaximal force repeatedly over a sustained period of time. In a study conducted by Biering-Sorenson in 1984, it was discovered that patients with low back pain had reduced levels of muscular endurance in the lumbar extensors in comparison with non-sufferers, recent research by authors such as Andersen (2007) supports this as they showed a similar association in a large sample of healthcare workers and students.
Studies have also reported that abdominal muscular endurance in low back pain sufferers is significantly decreased in contrast to those in the normal health population (Foster & Fulton, 1991), although a more recent study by Lewis (2009) showed that adolescents with LBP presented with significantly higher trunk flexor muscle endurance compared to adolescents without LBP. The argument is made that the ratio between flexor’s and extensor’s muscular endurance is more important in terms of LBP than endurance and strength measurements alone (Barr et al. 2007). The increase in flexion endurance and decrease in extension endurance, could be linked to having a poor posture and loss of the neutral position, therefore leading to LBP. (Freeman et al,2010)
Lumbar fatigue as a result of low muscular endurance has been shown to reduce the person’s ability to sense the positioning of the lumbar spine and that 25% of people with chronic LBP (n=57) had severely impaired ability in controlling the position of the lumbar spine after a fatiguing task.(Tamiela et al, 1999) This loss of control again links back to the fact that not being able to hold a neutral position is strongly associated with LBP. (freeman et al, 2010)
Physiologically in patients with lower back pain it has been shown they have a higher percentage of fast type I glycolytic fibres compared to the slow oxidative fibres, this can be expected to render them less resistant to fatigue, where-as non LBP people have a much higher percentage of the type II glycolytic fibres giving them better muscular endurance helping prevent lower back pain. (Mannion et al, 1997)
Muscular Strength [edit | edit source]
is the ability to exert a maximal force against a resistance. Several arguments can be made to suggest that this component of fitness has a large roll to play in low back pain. This is discussed further down the page
Addison, R. (1980). Trunk strength in patients seeking hospitalization for chronic low-back disorders. Spine, 5, 539-544.
Kravitz, L., & Andrews, R. (1995). Fitness & the low back. IDEA Today, 13(4), 44-52.
Body Composition [edit | edit source]
This is the relative amounts of muscle, fat, bone and other vital organs in the body. The prevalence of low back is undoubtedly related most commonly with body fat content/obesity. Numerous studies have been conducted highlighting the relationship between increased fat content and the likelihood/prevalence of lower back pain. A study conducted in 2003 [11] found that there was a moderate positive relationship between obesity and lower back pain, however the results were based on the BMI calculation which does not definitively measure body fat content. In a study conducted by Urquhart 2011 [12] , it was also evident that there was a relationship between obesity and lower back pain. The difference with this study however is that not only was the BMI calculation used as a measure of obesity but Lean Fat Mass and Lean Muscle Mass were also calculated to determine whether it was fat content or general increase weight that was directly proportional to the potential for LBP. It is the common belief that an increase in body weight alters spinal biomechanics and loading creating excess strain to be put through certain structures. The theory behind why back pain was less prevalent in those with high lean muscle mass was that the increase muscle mass was there to compensate for the excess spinal loading and therefore would not alter loading mechanics. The studies conducted however have all been cross-sectional studies and longitudinal studies will need to be completed to assess if a higher fat mass predisposes the development of lower back pain later in life. There has been a meta-analysis completed [13] reviewing the literature surrounding obesity and low back pain. In the cross-sectional studies analysed, there was a strong link between obesity and increased prevalance of LBP in the last 12 months, subjects seeking LBP care and chronic LBP sufferers. There was an increase in prevalance for overweight subjects in comparison with the non-overweight subjects however subjects classified as obese had the highest incidence rate of LBP. Of the cohort studies there was only a relationship highlighted between obesity on LBP. Results were adjusted for publication bias and only studies who controlled for potential confounding variables were included. The results remained the same after being subjected to these criterion. There have also been a number of studies investigating the relationship between bone mineral density (BMD) and the predisposition to low back pain. In a study conducted in 2011 [14] ,relationships were discovered between positional asymmetry, motion restriction and objective measurable increases in the BMD of affected vertebrae. Further on this page it will be explained how positional asymmetry and motional restriction can predispose people to LBP. Increased BMD was also found in the subjects suffering from chronic LBP however due to the inherently small differences in density the evidence could well have been circumstantial. Further investigations are required to assess the reproductability of the results and to clarify the reasoning for the increased BMD.
Flexibility[edit | edit source]
This is the range of movement available at any particular joint of the body. Patients presenting with low back pain often display significant reductions in degrees of several movements at the pelvis and trunk. Adequate flexibility of the lumbar spine enhances functional mechanical advantage, while spasmodic or shortened back muscles adversely affect spinal mechanics (Farfan, 1975) . Tightness in the hip flexors can reduce pelvic mobility and therefore put excess strain on the lumbar spine during certain disciplines of movement – especially into flexion, following that, tight hamstring and hip extensors can also contribute to a reduction in the lordotic curve, which can potentially effect spinal loading mechanisms and lead to injury(Foster and Fulton 1991) (Plowman 1992) . The relationship between flexibility and lower back pain however is still largely based around theory and there are yet to be a number of high quality experiments/investigations to either support or refute this hypothesis.
Strength and Low Back pain [edit | edit source]
Muscle strength is the contractile force a muscle is able to produce.
The large muscles of the back (See anatomy section) are often thought of as synomous with back strength. ( [15] ) It is a commonly held belief that having 'strong' back muscles will support the back and prevent back pain however there is conjecture in the literature surrounding this theory.
Many common exercises such as prone extensions, dead lifts and low-rows are thought to strengthen the back muscles and 'stabalise' the spine or prevent injury. Muscle strengthening exercises form part of the NICE treatment guidelines for Early management of persistent non-specific low back pain ( [16] ).

This section will look to;
- Introduce different methods of measuring back strength
- Evaluate the literature surrounding the area
- Summarise the findings
Measures of back strength [edit | edit source]
There are a variety of measures targeted at assessing muscular strength e.g. one rep max, isokinetic dynamometry, manual muscle testing etc.
Muscle strength with regards to the lower back is commonly researched as a proxy measure of ‘physical capacity’ which also includes muscle endurance and joint mobility ( [17] ) although there is a lack of sufficient high quality evidence surrounding reproducibility of current physical capacity measures in healthy subjects and in patient groups. ( [18] ).

When researching lower back strength in relation to prevalence of LBP, isokinetic maximal flexion and extension, calculated with an isokinetic dynamometer, isoinertial dynamic testing and isokinetic lifting force are commonly used ( [19] There is some evidence to show that isokinetic measurement is reproducible and valid ( [20] )
Evidence review [edit | edit source]
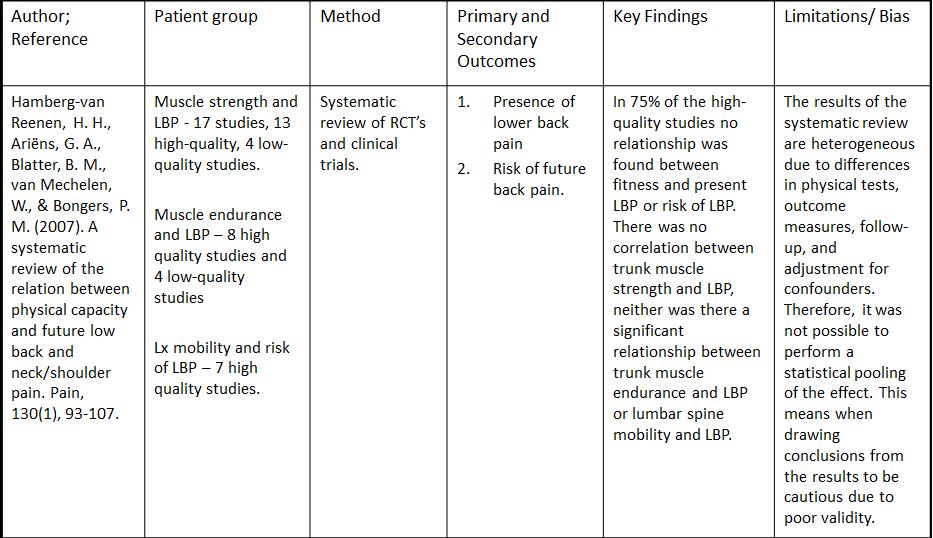
A systematic review from 2007 [17] evaluated evidence on the relationship between physical capacity and future low back and neck/shoulder pain. It was the first systematic review of longitudinal studies assessing the link between physical capacity and LBP.
Thirteen high quality studies reported no association between trunk muscle strength and future risk of low back pain. The risk ratios were insignificant between low and high isometric strength (0.6 and 1.2 respectively), however five high quality studies have shown that poor trunk muscle strength is a significant predictor of LBP and two other high quality studies found high strength as a risk factor. The results of this systematic review therefore are inconclusive one way or another in terms of the relationship between trunk strength and LBP. The review is further summaried in the table below.
A more recent study looking into LBP in male adolescents found isometric and isoinertial trunk performance was not significantly associated with LBP although they did find that regular sport participation was associated with LBP (93.9%:67.9% LBP + sport: No LBP + sport) [21] .
Another paper by [15] evaluating the strength and cross sectional area of extensor muscles in chronic LBP patients states that ‘weakness of the back muscles can lead to LBP’. The evidence this paper has used to support their own research actually contradicts the basis of their paper and is highlighted here as a good example of low quality research in the area based on commonly held beliefs rather than evidence based theory.
Clinical Relevence[edit | edit source]

The research is inconclusive with regards to strength and low back pain however there is good evidence that poor trunk muscle strength is a risk factor for LBP. The evidence has so far failed to establish causality. Clinical guidance e.g. NICE guidelines still recommend strength exercises as part of a rehab program for BP.
Bottom Line[edit | edit source]
An argument can be made for or against using strengthening exercises as a preventative measure for back pain More high quality research is needed to determine if either low or high strength is a risk factor for LBP. = Sub Heading 2 = == Sub Heading 3 == == Recent Related Research (from Pubmed) ==
== References == References will automatically be added here, see adding references tutorial.
- ↑ Palmer KT, Walsh K, et al. Back pain in Britain: comparison of two prevalence surveys at an interval of 10 years BMJ 2000
- ↑ Helliovaara, M. Risk factors for low back pain and sciatica. Annals of Medicine.1989
- ↑ Clinical Standards Advisory Group. NHS 1994
- ↑ The Royal College of General Practitioners. fckLRfckLRDiagnostic Triage Flow Chart of a patient presenting with low back pain with or without leg pain. Found at : http://www.chiro.org/LINKS/GUIDELINES/FULL/Royal_College/backpain12.html
- ↑ Hayden J, van Tulder MW, Malmivaara A, Koes BW. Exercise therapy for treatment of non-specific low back pain. Cochrane Database of Systematic Reviews 2005
- ↑ President's Council on Physical Fitness and Sports: Physical Fitness Research Digest. Series 1,No.1, Washington DC,1971.
- ↑ Mota, Jorge, et al. "Association of maturation, sex, and body fat in cardiorespiratory fitness." American Journal of Human Biology 14.6 (2002): 707-712.
- ↑ Stark, Timothy, et al. "Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: a systematic review." PM&amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;R 3.5 (2011): 472-479.
- ↑ Wilson, J. P., Mulligan, K., Fan, B., Sherman, J. L., Murphy, E. J., Tai, V. W., ... &amp;amp;amp;amp; Shepherd, J. A. (2012). Dual-energy X-ray absorptiometry–based body volume measurement for 4-compartment body composition. The American journal of clinical nutrition, 95(1), 25-31.
- ↑ Mohamed, Abeer A., et al. "Comparison of Strain-Gage and Fiber-Optic Goniometry for Measuring Knee Kinematics During Activities of Daily Living and Exercise." Journal of biomechanical engineering 134.8 (2012).
- ↑ Bener, A., Alwash, R., Gaber, T. and Lovasz,G. 2003. Obesity and Low Back Pain. Coll. Antropol. 27 (2003) 1: 95–104
- ↑ Urquhart, D.M. 2011, Higher Body Fat Linked to Increased Back Pain. Spine 9/1/2011 Edition. Lippincott Williams and Wilkins, Philadelphia
- ↑ Shiri, R., Karppinen, J., Leino-Arjas, P., Solovieva, S., &amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp; Viikari-Juntura, E. (2010). The association between obesity and low back pain: a meta-analysis. American journal of epidemiology, 171(2), 135-154.
- ↑ Snider, K. T., Johnson, J. C., Degenhardt, B. F., &amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp;amp; Snider, E. J. (2011). Low back pain, somatic dysfunction, and segmental bone mineral density T-score variation in the lumbar spine. The Journal of the American Osteopathic Association, 111(2), 89.fckLRChicago
- ↑ 15.0 15.1 Lee HJ, Lim WH, Park JW, Kwon BS, Ryu KH, Lee JH, Park YG. The Relationship between Cross Sectional Area and Strength of Back Muscles in Patients with Chronic Low Back Pain. Ann Rehabil Med. 2012
- ↑ NICE : CG88 Low back pain: Early management of persistent non-specific low back pain 2009
- ↑ 17.0 17.1 Hamberg-van Reenen HH, Ariëns GAM, Blatter BM, Mechelen W, Bongers PM. A systematic review of the relation between physical capacity and future low back and neck/shoulder pain. Pain. 2007
- ↑ Essendrop M, Maul I, Läubli T, Riihimäki H, Schibye B. Measures of low back function: a review of reproducibility studies. Clinical Bio-mechanics (Bristol, Avon). 2002
- ↑ Takala E P, Viikari‐Juntura E. Do functional tests predict low back pain? Spine 2000
- ↑ Dvir Z, Keating J. The reproducibility of isokinetic trunk extension: a study using very short range of motion. 2001 Clin Biomech
- ↑ Balagué F, Bibbo E, Mélot C, Szpalski M, Gunzburg R, Keller TS. The association between isoinertial trunk muscle performance and low back pain in male adolescents. Eur Spine J. 2010;
</div>

