Plantar Fasciitis: Difference between revisions
Elien Lebuf (talk | contribs) No edit summary |
Elien Lebuf (talk | contribs) No edit summary |
||
| Line 147: | Line 147: | ||
=== [[Image:16215944 10211611117223808 2067350409 n.png|border|center]]5. Taping<br> === | === [[Image:16215944 10211611117223808 2067350409 n.png|border|center]]5. Taping<br> === | ||
Recent searches were done toward the effects of short-term treatment with kinesiotaping for plantar fasciitis. For an entire week the tape was placed on the gastrocnemius and the plantar fascia. It was concluded that the additional treatment with continuous kinesiotaping for one week might alleviate the pain of plantar fasciitis better than a traditional physical therapy program only, but it’s a short-time effect. [http://www.physio-pedia.com/Windlass_test The windlass mechanism] describes the manner by which the plantar fascia supports the foot during weight- bearing activities and provides information regarding the biomechanical stresses placed on the plantar fascia. To assess the efficacy of a taping construction as an intervention or as part of an intervention in patients with plantar fasciitis on pain and disability, controlled trials were searched for in CINAHL, EMBASE, MEDLINE, Cochrane CENTRAL, and PEDro using a specific search strategy. The Physiotherapy Evidence Database scale was used to judge methodological quality. Clinical relevance was assessed with five specific questions. A best-evidence synthesis consisting of five levels of evidence was applied for qualitative analysis. [24][25][26](level 1A)<br><br>Taping for plantar fasciitis can decrease pain by distributing the force away from the strained plantar fascia. The NISMAT recommends a tape technique shown in 5 steps with a 1 inch tape.<br> | Recent searches were done toward the effects of short-term treatment with kinesiotaping for plantar fasciitis. For an entire week the tape was placed on the gastrocnemius and the plantar fascia. It was concluded that the additional treatment with continuous kinesiotaping for one week might alleviate the pain of plantar fasciitis better than a traditional physical therapy program only, but it’s a short-time effect. [http://www.physio-pedia.com/Windlass_test The windlass mechanism] describes the manner by which the plantar fascia supports the foot during weight- bearing activities and provides information regarding the biomechanical stresses placed on the plantar fascia. To assess the efficacy of a taping construction as an intervention or as part of an intervention in patients with plantar fasciitis on pain and disability, controlled trials were searched for in CINAHL, EMBASE, MEDLINE, Cochrane CENTRAL, and PEDro using a specific search strategy. The Physiotherapy Evidence Database scale was used to judge methodological quality. Clinical relevance was assessed with five specific questions. A best-evidence synthesis consisting of five levels of evidence was applied for qualitative analysis. [24][25][26](level 1A)<br><br>Taping for plantar fasciitis can decrease pain by distributing the force away from the strained plantar fascia. The NISMAT recommends a tape technique shown in 5 steps with a 1 inch tape.<br> | ||
#Place anchor strips: one goes around the distal part of the metatarsals. The other covers the medial and lateral borders of the foot. (fig. 9) | |||
#Start at the fifth metatarsal head, follow the lateral border up, then come around the calcaneus and across to finish where started. (fig. 10) | |||
#Repeat number two but starting and finishing at the first metatarsal head. (fig. 11) | |||
#Alternate this arch crossing three times each way (fig. 12) | |||
#Finish by covering the anchor strips with two more anchor strips (fig. 13)34 | |||
<br> | <br> | ||
| Line 153: | Line 159: | ||
But in an RCT by Matthew R. et al they have proven that calcaneal taping resulted in a greater reduction in pain than stretching or sham taping. This technique inverts the heel to raise the medial longitudinal arch of the foot. After two treatment sessions the technique resulted in a significantly greater reduction in pain than stretching or sham taping. | But in an RCT by Matthew R. et al they have proven that calcaneal taping resulted in a greater reduction in pain than stretching or sham taping. This technique inverts the heel to raise the medial longitudinal arch of the foot. After two treatment sessions the technique resulted in a significantly greater reduction in pain than stretching or sham taping. | ||
[[Image:16237581 10211611117183807 90377099 n.png|border|center]]Applying a calcaneal taping (figure14): A Corver-roll is applied to a clean and dry skin and then covered with leukotape. (1A | [[Image:16237581 10211611117183807 90377099 n.png|border|center]]<br>Applying a calcaneal taping (figure14): A Corver-roll is applied to a clean and dry skin and then covered with leukotape. (1A)<br> | ||
#The first piece is applied just distal to the lateral malleolus over the calcaneus and attached distal to the malleolus medialis. The calcaneus will be pulled more medially. (1B) | |||
#Piece two and three are applied in the same way and covering one third of the tape more distal to the calcaneus. (1C and 1D) | |||
#Piece four Starts distal at the malleolus lateralis and is wrapping around the posterior aspect of the calcaneus to the distal part of malleolus medialis (1E). This serves as an anchor for the first three pieces. (1F)28 (level 1B)<br> | |||
== Clinical bottom line<br> == | == [[Image:16216199 10211611117263809 668222733 n.png|border|center]]Clinical bottom line<br> == | ||
Plantar fasciitis is one of the most common causes of heel pain. [48] Hereby, it is important to know the risk factors for patients and the outcomes of the physical examination, which can guide you to classify the patient into plantar fasciitis. Most patients with plantar fasciitis are aided with conservative methods as we discussed above. | Plantar fasciitis is one of the most common causes of heel pain. [48] Hereby, it is important to know the risk factors for patients and the outcomes of the physical examination, which can guide you to classify the patient into plantar fasciitis. Most patients with plantar fasciitis are aided with conservative methods as we discussed above. | ||
| Line 254: | Line 262: | ||
[[Category:Vrije_Universiteit_Brussel_Project|Template:VUB]] [[Category:EIM_Residency_Project]] [[Category:Foot]] [[Category:Musculoskeletal/Orthopaedics]] | [[Category:Vrije_Universiteit_Brussel_Project|Template:VUB]] [[Category:EIM_Residency_Project]] [[Category:Foot]] [[Category:Musculoskeletal/Orthopaedics]] | ||
<br> | |||
Revision as of 23:01, 24 January 2017
Original Editors
Top Contributors - Admin, Kris Porter, Rachael Lowe, Elien Lebuf, Bert Pluym, Esraa Mohamed Abdullzaher, Kim Jackson, Chrysolite Jyothi Kommu, Jonathan Wong, Brooke Kennedy, Lucinda hampton, Scott Buxton, Olajumoke Ogunleye, Jeroen Van Cutsem, Thomas Janicky, Elke Lathouwers, Vidya Acharya, Aminat Abolade, Kai A. Sigel, Lisa Couck, Khloud Shreif, Simisola Ajeyalemi, Tony Lowe, Jarapla Srinivas Nayak, Keta Parikh, Stijn Van de Vondel, Habibu Salisu Badamasi, WikiSysop, Rishika Babburu, Padraig O Beaglaoich, Jessica Galasso, Sehriban Ozmen, Yahya Al-Razi, Shaimaa Eldib, Saud Alghamdi, Claire Knott, David Csepe, Wanda van Niekerk and Jess Bell
Original Editor - Brooke Kennedy
Top Contributors - Admin, Kris Porter, Rachael Lowe, Elien Lebuf, Bert Pluym, Esraa Mohamed Abdullzaher, Kim Jackson, Chrysolite Jyothi Kommu, Jonathan Wong, Brooke Kennedy, Lucinda hampton, Scott Buxton, Olajumoke Ogunleye, Jeroen Van Cutsem, Thomas Janicky, Elke Lathouwers, Vidya Acharya, Aminat Abolade, Kai A. Sigel, Lisa Couck, Khloud Shreif, Simisola Ajeyalemi, Tony Lowe, Jarapla Srinivas Nayak, Keta Parikh, Stijn Van de Vondel, Habibu Salisu Badamasi, WikiSysop, Rishika Babburu, Padraig O Beaglaoich, Jessica Galasso, Sehriban Ozmen, Yahya Al-Razi, Shaimaa Eldib, Saud Alghamdi, Claire Knott, David Csepe, Wanda van Niekerk and Jess Bell
Topic Expert - Kris Porter
Search Strategy
[edit | edit source]
We searched scientific articles and more information by using the websites PubMed, Web of Science, Google Scholar and PEDro. We used the keywords: “plantar fasciitis”, “rehabilitation”, “physiotherapy”, “plantar fasciosis” and “plantar heel pain”.
Definition/Description[edit | edit source]
Plantar fasciitis may be referred to as plantar fasciosis, plantar heel pain, plantar fascial fibramatosis, among others. The pathology that is usually present in the medial heel region has traditionally been known as plantar fasciitis. However, recently, the term plantar fasciosis has been used to dismiss the inflammatory component and emphasize the degenerative nature that is observed histologically in the insertion zone in the calcaneus [34]. The fact that many cases diagnosed as “plantar fasciitis” are not inflammatory conditions, and thus should be referred to as "plantar fasciosis”, is confirmed through histological analysis which demonstrates plantar fascia fibrosis, collagen cell death, vascular hyperplasia, random and disorganized collagen, and avascular zones [2]. There are many different sources of pain in the plantar heel besides the plantar fascia, and therefore the term "Plantar Heel Pain" serves best to include a broader perspective when discussing this and related pathology.
Anatomy[edit | edit source]
The plantar fascia is comprised of white longitudinally organized

fibrous connective tissue which originates on the periosteum of the medial calcaneal tubercle, where it is thinner but it extends into a thicker central portion. The thicker central portion of the plantar fascia then extends into five bands surrounding the flexor tendons as it passes all 5 metatarsal heads. The plantar fascia blends with the paratenon of the Achilles tendon, the intrinsic foot musculature and even the skin and subcutaneous tissue.[2][3] The thick viscoelastic multilocular fat pad is responsible for absorbing up to 110% of body weight during walking and 250% during running and deforms most during barefoot walking vs. shod walking.[4]
Pain in the plantar fascia can be insertional and/or non-insertional and may involve the larger central band, but may also include the medial and lateral band of the plantar fascia. The plantar fascia is best referred to as fascia because of it's relatively variable fiber
orientation as opposed to the more linear fiber orientation of aponeurosis.[49]
Epidemiology & Etiology
[edit | edit source]
Epidemiology[edit | edit source]
The prevalence of pain in the hind foot and region of the heel is high in both athletic and non athletic regions. Although it occurs more frequently in running-related activities such as running,soccer and gymnastics. [39]
Although this condition is seen in all ages, it is most commonly experienced during the age between 20 and 34 years old.[40]
Plantar fasciitis accounted for 8% of the reported previous overuse, with a greater incidence in female runners. [11,59]
Etiology[edit | edit source]
There are many risk factors which contribute to plantar heel pain :
Presence of limited ankle dorsiflexion range of motion, high body mass index in nonathletic individuals, running and work-related weight-bearing activities, particularly under conditions with poor shock absorption [46]
Risk factors in runners are, street running, spiked shoes and hind-foot varus [42] , an increased height (57). Greater rates of increase in vertical ground reaction forces and a lower medial longitudinal arch where found in female runners (56).
In an nonathletic population a strong association is found between a higher body mass index and plantar heel pain (43), also work-related weight-bearing activities such as prolonged standing on hard surfaces, walking and number of times jumping in and out of vehicles (60).
Characteristics/Clinical Presentation[edit | edit source]
Heel pain/plantar fasciitis usually presents as a chronic condition, with symptom duration greater than one year prior to seeking treatment. The mean duration of symptoms last longer than 6 months (8,10,50,52,61).
Plantar medial heel pain, most noticeable with initial steps after a period of inactivity (46)
A typical presentation of the pain is early in the morning. Once starting walking, the pain tends to recede, but never fully resolves throughout the course of the day (50).
Pain is worse following prolonged weight bearing, such as prolonged walking or exercise, particularly on hard surfaces (46).
Nonathletic individuals present often with a high body mass index. (43)
Differential Diagnosis
[edit | edit source]
Differential diagnosis is complex, as there may be pain from more than one structure.
Possible other sources of medial heel pain are fat pad atrophy(61), calcaneal apophysis in adolescents (58), tibialis posterior dysfunction (54), proximal plantar fibroma (51), neural sources like S1 radiculopathy and tarsal tunnel syndrome (58), stress fractures (calcaneum, talus and navicular bone), plantar fascia rupture and rheumatological diseases (53)
Diagnostic Procedures[edit | edit source]
Plantar fasciitis is a clinical diagnosis. It is based on patient history and physical exam. Therefore, there are a couple of risk factors which the examiner has to bear in mind while examining the patient fort he first time. These are the presence of limited ankle dorsiflexion range of motion, high body mass index in nonathletic individuals, running, and work-related weight-bearing activities. [46] (level 1A)
Also one of the most important clinical findings us pain in the plantar medial heel region (most noticable in the morning, the first staps after a period of inactivity or after prolonged weight bearing activities) [46, 47, 48]
There is a possibility of using imaging diagnostics, but it is not recommended for the initial evaluation. However, imaging such as MRI can be required to rule out other considerations in the differential diagnosis. [48] (level 1A)
Outcome Measures[edit | edit source]
- The FAAM, or Foot and Ankle Ability Measure, is a good outcome measure to give to patients that are diagnosed with plantar fascitis.
- The Foot Function Index, or FFI but only the the pain subscale. It is a validated measure, and the first 7 items of the pain subscale are used as the primary numeric outcome measure. Items are scored from 0 (no pain) to 10 (worst pain imaginable) depending on the mark on the visual analog scale. The sum of the 7 items is then expressed as a percentage of maximum possible score, ranging in an overall percentage.
- The foot health status questionnaire
- The Bristol foot score can be used for assess the patient’s perception of the impact of foot problems on everyday life. It’s also a relevant questionnaire to determine satisfaction of foot orthotics.. There are 15 questions: foot concern and pain (7), footwear and general foot health (4) and mobility (3).
- The foot health status questionnaire, or FHSQ can be used to assess the effects of footwear and orthotic interventions (30).
Examination[edit | edit source]
The clinical examination will take under consideration a patient's medical history, physical activity, foot pain symptoms and more. The doctor may decide to use imaging studies like radiographs, diagnostic ultrasound and MRI.
Fabrikant et al could conclude that office-based ultrasound can help diagnose and confirm plantar fasciitis/fasciosis through the measurement of the plantar fascia thickness. Because of the advantages of ultrasound-that it is non-invasive with greater patient acceptance, cost effective and radiation-free-the imaging tool should be considered and implemented early in the diagnosis and treatment of plantar fasciitis/fasciosis. [13] (level 3)
Sutera et al found that imaging the ankle/hind foot in the upright weight-bearing position with a dedicated MR scanner and a dedicated coil might enable the identification of partial tears of the plantar fascia, which could be overlooked in the supine position. [14] (level 3)
Risk factors to look for by the examination of plantar fasciitis are:
- Limited active and passive talocrural joint dorsiflexion range of motion
- Obesity or high body mass index in nonathletic individuals
- Work-related weight-bearing
These findings also indicate the diagnosis of plantar fasciitis [46] (level 1A):
- Plantar medial heel pain: most noticeable with initial steps after a period of inactivity but also worse following prolonged weight bearing
- Active and passive talocrural joint dorsiflexion range of motion
- Pain with palpation of the proximal insertion of the plantar fascia
- Positive windlass test
- Negative tarsal tunnel tests (Tinel's test, for further information see tarsal tunnel syndrome)
- Abnormal FPI score
- The longitudinal arch angle
Medical Management
[edit | edit source]
Plantar fasciitis frequently responds to a broad range of conservative therapies. Modalities commonly used include rest, ice massage, stretching of the Achilles tendon and plantar fascia, nonsteroidal anti-inflammatory medications (NSAIDs), corticosteroid injections, foot padding, taping, shoe modifications (steel shank and anterior rocker bottom), arch supports, heel cups, custom foot orthoses, night splints, ultrasound, and casting [36, 38].
The use of oral NSAID’s in treatment for plantar fasciitis has proven to be significantly helpful in improving pain and disability. Pain and disability mean scores improve significantly over time with use of NSAID’s. There was a trend towards improved pain relief and disability, especially in the interval between the 2 and 6- month follow-up. Pain improved from baseline to 6 months by a factor of 5.2 and disability by 3.8. These results are quantified by using the Foot Function Index [36].
Other forms of conservative therapy used for treating acute plantar fasciitis include use of corticosteroid injections and ultrasound therapy. When used, pain intensity may reduce significantly.
However, the pain reduction achieved by corticosteroid injection has been proven to be significantly greater when compared to pain relief after undergoing ultrasound therapy (p<.0001). Although corticosteroid injections have proven to be effective in treating heel pain, and has better therapeutic outcomes than ultrasound therapy, treatment failure occurs quite frequently (>30% of cases). When assessing pain reduction and functional outcomes, the improvements achieved by corticosteroid injections only seem to continue untill 12 weeks and thus does only cover acute symptoms [45, 46].
When conservative measures fail, surgical plantar fasciotomy with or without heel spur removal may be employed. There is a method, through an open procedure, percutaneously or most common endoscopically, that releases the plantar fascia. This is an effective treatment, without the need for removal of a calcaneal spur, when present. There is a professional consensus, 70-90% of heel pain patients can be managed by non-operative measures. Surgery for plantar fasciitis should be considered only after all other forms of treatment have failed. With an endoscopic plantar fasciotomy, using the visual analog scale, the average post-operative pain was improved from 9.1 to 1.6. For the second group (ESWT), using the visual analog scale the average post-operative pain was improved from 9 to 2.1. Endoscopic plantar fasciotomy gives better results than extra-corporeal shock wave therapy, but with liability of minor complications.[15][16]
Physical Therapy Management
[edit | edit source]
The most common treatments include stretching of the gastroc/soleus/plantar fascia, orthotics, ultrasound, iontophoresis, night splints, joint mobilization/manipulation, and surgery.
1. Stretching[edit | edit source]
Stretching Plantar fascia:
- The patient cross their affected leg over the contralateral leg and using the fingers across to the base of the toes to apply pressure into toe extension until a stretch can be felt along the plantar fascia. (figure 2)
- Step test: the patient position himself on a step with the ball of his foot and drops his heel while remaining the forefoot on the step. (figure 3)
- The patient can also use a towel to stretch the plantar fascia while sitting. The towel goes around the forefoot and the patient pulls the forefoot in dorsiflexion27 (level 1A). (figure 5)
- Rolling the foot (plantar fascia) over a tennis ball.28 (level 1B) (figure 4)

Stretching of the achilles tendon, soleus and gastrocnemius:
- The achilles tendon can be stretched in a standing position with the affected leg placed behind the contralateral legwith the toes pointed forward. The front knee was then bent, keeping the back knee straight and heel on the ground. In this position is the gastrocnemius stretched as well. (figure 6)
- If the patient wants to focus more on the soleus muscle, the back knee could then be in a flexed position[17](level 2B) . (figure 7)

2. Mobilizations and manipulations
[edit | edit source]
Mobilizations and manipulations have also been shown to decrease pain and relieve symptoms in some cases. Posterior talocrural joint mobs and subtalar joint distraction manipulation have been performed with the hypomobile talocrural joint. Patients in 6 different cases demonstrated complete pain relief and full return to activities with an average of 2-6 treatments per case[18] (level 4).
Patients also need to be examined for active trigger points in the gastrocnemius. The diagnosis guidelines:
- Presence of a palpable taut band.
- Presence of a hypersensitive area in the taut band.
- Local twitch response provoked by the snapping palpation of the taut band.
- Reproduction of referred pain in response to compression.
Technique for the treatment of trigger points:
- Trigger points pressure release technique Video pressure release technique
Pressure is applied on the trigger points until an increase in muscle resistance is perceived. This pressure will be maintained until the release of the taut band is examined. After the release the pressure need to be increased to return to previous level of muscle trigger point tension. This repeated for 90s consisting out 3 repetitions. - Neuromuscular technique (longitudinal stroke) Video neuromuscular technique
The patient is placed in prone position, the thumb of the therapist is placed over the taut band and 3 longitudinal strokes were performed from caudal (ankle) to cranial (knee).37 (level 1A)
3. Orthotics[edit | edit source]
Posterior-night splints maintain ankle dorsiflexion and toe extension, allowing for a constant stretch on the plantar fascia. Some evidence reports night splints to be beneficial but in a review by Cole et al he reported that there was limited evidence to support the use of night splints to treat patients with pain lasting longer than six months, and patients treated with custom made night splints improved more than prefabricated night splints[19] (level 3A).
In a meta-analyse from stadler et al. they compared the outcomes of 103 patients separated over three treatment categories: anti-inflammatory (corticosteroid injections), accommodative (viscoelastic heel cup) and mechanical (low-Dye taping for one month followed by rigid custom orthotics for two months). After three months of treatment 70% of the participants in the mechanical treatment group rated their outcome as "excellent" or "fair" compared to the other groups with only 30 - 33%.35 (level 1B) Foot orthoses can produce small short-term benefits in function and may also produce small reductions in pain for people with plantar fasciitis, but they do not have long-term beneficial effects compared with a sham device whether they are custom made or prefabricated[22] (level 1B).
Examples of orthotics for plantar fasciitis
- Over the counter heel cup
- Custom made foot orthotics: in a study of Roos et al. patients complained in the first week of pressure pain and tiredness of the foot (n = 3 of 13). But after 12 weeks there were no side effect examined, there was only one patient that complained of tiredness of the foot.
- Anterior/posterior night splint: in a study of Roos et al. patients who used the night splint reported in the first week side effects such as pressure pain and sleep disturbances (n = 9 of 15). But after 12 weeks there remained two to five patients with side effects.28 (level 1B)
4. Strength training
[edit | edit source]
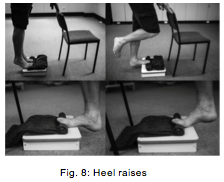
In a study by Rathleff, Michael Skovdal et al they showed that high load strength training is effective for the treatment of patients with plantar fasciitis (figure 8). This treatment consist of unilateral heel raises on a stairway or similar location with a towel under the toes to activate the windlass mechanism (see diagnostic procedures). The heel raises were performed 3s concentric (going up), 3s eccentric (going down) and 2s isometric pause at the top of the concentric phase. The exercise is performed every second day. The patients reported less foot pain and a significant FFI score after 3 months.30 (level 1B)
Scott K. Lynn et al. showed in a RCT by comparing two effective exercise therapies that short-foot exercise (SFE) are more effective than the towel curl exercise (TCE) at training the intrinsic foot musculature. Both therapies decreased the mediolateral center of pressure (MLCOP) however the SFE decreased the MLCOP much more than the TCE training.
- Short foot exercise: Raise the medial longitudinal arch of the foot, draw the metatarsal heads toward the calcaneus without flexing the toes, hold isometric for 5 seconds.
- Towel curl exercise: Place a towel on the floor with the toes on the border, drag the towel in 5 seconds under the foot by flexing the toes [35].
 5. Taping
5. Taping
[edit | edit source]

Recent searches were done toward the effects of short-term treatment with kinesiotaping for plantar fasciitis. For an entire week the tape was placed on the gastrocnemius and the plantar fascia. It was concluded that the additional treatment with continuous kinesiotaping for one week might alleviate the pain of plantar fasciitis better than a traditional physical therapy program only, but it’s a short-time effect. The windlass mechanism describes the manner by which the plantar fascia supports the foot during weight- bearing activities and provides information regarding the biomechanical stresses placed on the plantar fascia. To assess the efficacy of a taping construction as an intervention or as part of an intervention in patients with plantar fasciitis on pain and disability, controlled trials were searched for in CINAHL, EMBASE, MEDLINE, Cochrane CENTRAL, and PEDro using a specific search strategy. The Physiotherapy Evidence Database scale was used to judge methodological quality. Clinical relevance was assessed with five specific questions. A best-evidence synthesis consisting of five levels of evidence was applied for qualitative analysis. [24][25][26](level 1A)
Taping for plantar fasciitis can decrease pain by distributing the force away from the strained plantar fascia. The NISMAT recommends a tape technique shown in 5 steps with a 1 inch tape.
- Place anchor strips: one goes around the distal part of the metatarsals. The other covers the medial and lateral borders of the foot. (fig. 9)
- Start at the fifth metatarsal head, follow the lateral border up, then come around the calcaneus and across to finish where started. (fig. 10)
- Repeat number two but starting and finishing at the first metatarsal head. (fig. 11)
- Alternate this arch crossing three times each way (fig. 12)
- Finish by covering the anchor strips with two more anchor strips (fig. 13)34
But in an RCT by Matthew R. et al they have proven that calcaneal taping resulted in a greater reduction in pain than stretching or sham taping. This technique inverts the heel to raise the medial longitudinal arch of the foot. After two treatment sessions the technique resulted in a significantly greater reduction in pain than stretching or sham taping.

Applying a calcaneal taping (figure14): A Corver-roll is applied to a clean and dry skin and then covered with leukotape. (1A)
- The first piece is applied just distal to the lateral malleolus over the calcaneus and attached distal to the malleolus medialis. The calcaneus will be pulled more medially. (1B)
- Piece two and three are applied in the same way and covering one third of the tape more distal to the calcaneus. (1C and 1D)
- Piece four Starts distal at the malleolus lateralis and is wrapping around the posterior aspect of the calcaneus to the distal part of malleolus medialis (1E). This serves as an anchor for the first three pieces. (1F)28 (level 1B)
 Clinical bottom line
Clinical bottom line
[edit | edit source]

Plantar fasciitis is one of the most common causes of heel pain. [48] Hereby, it is important to know the risk factors for patients and the outcomes of the physical examination, which can guide you to classify the patient into plantar fasciitis. Most patients with plantar fasciitis are aided with conservative methods as we discussed above.
[edit | edit source]
Miller et al. 2015[55]
Unfortunately, the effectiveness of continued conservative treatment for inferior heel pain diminishes if symptoms have not reduced with 3-6 months of standard treatment. Invasive surgical options have moderate patient succes rates, extended recovery times, and potential complications. Given the growing evidence for the role of local hemodynamics in chronic plantar fasciitis, therapies intended to stimulate angiogenesis and.or improve local circulation (which may revert a chronic lesion to an acute lesion by stimulating the inflammatory phase of the healing cascade.) have recently been explored with promising results.
Extracorporeal shockwave therapy remains a controversial therapy.
Radiofrequency microtendotony : stimulates angiogenesis in the avascular, fibrotic fascia, which promotes secretion of fibroblastic growth factor, vascular endothelical growth factor and vascular cells. Several case series have reported promising outcomes in recalcitrant plantar fasciitis with the open method more efficacious than the percutaneous technique. Follow-up data is limited to 1 year or less in all studies.
Platelet rich plasma(PRP) injections :
Prp is an autologous biological blood-derived product that contains high concentrations of plateled- derived growth factor. Soft tissue healing is thought to be stimulated via enhanced fibroblast migration and proliferation, up regulated vascularisation, and increased collagen deposition. Case series with no more than 1 year follow-up have reported pain severity improvement of 45% at 6 months.
Micromobile Compression (MMC)
MMC is a non-invasive technology that augments circulation through the deep veins of the leg via cyclic pressure pulses to the plantar venous plexus. The platform for the MMC is an orthotic that provides cyclic compression to the arch of the foot when the user is non-weight bearing. MMC has been attempted only on one patient, but further research is planned from 2015, to further evaluate the potential of MMC for plantar fasciitis.
Key Research[edit | edit source]
DiGiovanni BF, Nawoczenski DA, Lintal ME et al. Tissue-specific plantar fascia stretching exercises enhances outcomes in patients with chronic heel pain. Journal of Bone and Joint Surgery. 2003;85-A:1270-1277.
According to a prospective, randomized controlled trial by DiGiovanni, stretching can be an appropriate treatment for plantar fascitis as long as it is specific stretching. He compared patients who received either a plantar-fascia tissue-stretching program compared to patients who received an achilles tendon stretching program. The plantar fascia stretching consisted of one stretch to be performed before taking their first step in the morning. The patient crossed the affected leg over the contralateral leg and used the fingers across to the base of the toes to apply pressure into toe extension until a stretch was felt along the plantar fascia. In the achilles-tendon stretching group, the stretch was performed in a standing position and to be performed immediately after getting out of bed in the morning. A shoe insert was placed under the affected foot, and the affected leg was placed behind the contralateral leg with the toes pointed forward. The front knee was then bent, keeping the back knee straight and heel on the ground. Both stretches for both groups were to be held 10 secondes for 10 repetitions, 3 times a day. The results indicated that both groups improved but the planta fascia specific stretching was superior. The protocol was linked to the use of dorsiflexion night splints that incorporate toe dorsiflexion, but reported the stretching program had advantages over night splints.
Pfeffer G, Bacchetti P, Deland J et al. Comparison of custom and prefabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot Ankle Int. 1999 Apr;20(4):214-21.
Abstract
Fifteen centers for orthopaedic treatment of the foot and ankle participated in a prospective randomized trial to compare several nonoperative treatments for proximal plantar fasciitis (heel pain syndrome). Included were 236 patients (160 women and 76 men) who were 16 years of age or older. Most reported duration of symptoms of 6 months or less. Patients with systemic disease, significant musculoskeletal complaints, sciatica, or local nerve entrapment were excluded. We randomized patients prospectively into five different treatment groups. All groups performed Achilles tendon- and plantar fascia-stretching in a similar manner. One group was treated with stretching only. The other four groups stretched and used one of four different shoe inserts, including a silicone heel pad, a felt pad, a rubber heel cup, or a custom-made polypropylene orthotic device. Patients were reevaluated after 8 weeks of treatment. The percentages improved in each group were: (1) silicone insert, 95%; (2) rubber insert, 88%; (3) felt insert, 81%; (4)stretching only, 72%; and (5) custom orthosis, 68%. Combining all the patients who used a prefabricated insert, we found that their improvement rates were higher than those assigned to stretching only (P = 0.022) and those who stretched and used a custom orthosis (P = 0.0074). We conclude that, when used in conjunction with a stretching program, a prefabricated shoe insert is more likely to produce improvement in symptoms as part of the initial treatment of proximal plantar fasciitis than a custom polypropylene orthotic device.
Osborne HR, Allison GT. Treatment of plantar fasciitis by LowDye taping and iontophoresis: short term results of a double blinded, randomised, placebo controlled clinical trial of dexamethasone and acetic acid. Br J Sports Med. 2006 Jun;40(6):545-9; discussion 549. Epub 2006 Feb 17.
OBJECTIVES: To determine if, in the short term, acetic acid and dexamethasone iontophoresis combined with LowDye (low-Dye) taping are effective in treating the symptoms of plantar fasciitis. METHODS: A double blinded, randomised, placebo controlled trial of 31 patients with medial calcaneal origin plantar fasciitis recruited from three sports medicine clinics. All subjects received six treatments of iontophoresis to the site of maximum tenderness on the plantar aspect of the foot over a period of two weeks, continuous LowDye taping during this time, and instructions on stretching exercises for the gastrocnemius/soleus. They received 0.4% dexamethasone, placebo (0.9% NaCl), or 5% acetic acid. Stiffness and pain were recorded at the initial session, the end of six treatments, and the follow up at four weeks. RESULTS: Data for 42 feet from 31 subjects were used in the study. After the treatment phase, all groups showed significant improvements in morning pain, average pain, and morning stiffness. However for morning pain, the acetic acid/taping group showed a significantly greater improvement than the dexamethasone/taping intervention. At the follow up, the treatment effect of acetic acid/taping and dexamethasone/taping remained significant for symptoms of pain. In contrast, only acetic acid maintained treatment effect for stiffness symptoms compared with placebo (p = 0.031) and dexamethasone. CONCLUSIONS: Six treatments of acetic acid iontophoresis combined with taping gave greater relief from stiffness symptoms than, and equivalent relief from pain symptoms to, treatment with dexamethasone/taping. For the best clinical results at four weeks, taping combined with acetic acid is the preferred treatment option compared with taping combined with dexamethasone or saline iontophoresis.
Cole C, Seto C, Gazewood J. Plantar fasciitis: evidence-based review of diagnosis and therapy. Am Fam Physician. 2005 Dec 1;72(11):2237-42.
Plantar fasciitis causes heel pain in active as well as sedentary adults of all ages. The condition is more likely to occur in persons who are obese or in those who are on their feet most of the day. A diagnosis of plantar fasciitis is based on the patient's history and physical findings. The accuracy of radiologic studies in diagnosing plantar heel pain is unknown. Most interventions used to manage plantar fasciitis have not been studied adequately; however, shoe inserts, stretching exercises, steroid injection, and custom-made night splints may be beneficial. Extracorporeal shock wave therapy may effectively treat runners with chronic heel pain but is ineffective in other patients. Limited evidence suggests that casting or surgery may be beneficial when conservative measures fail.
Landorf KB, Keenan AM, Herbert RD. Effectiveness of foot orthoses to treat plantar fasciitis: a randomized trial. Arch Intern Med. 2006 Jun 26;166(12):1305-10.
BACKGROUND: Plantar fasciitis is one of the most common foot complaints. It is often treated with foot orthoses; however, studies of the effects of orthoses are generally of poor quality, and to our knowledge, no trials have investigated long-term effectiveness. The aim of this trial was to evaluate the short- and long-term effectiveness of foot orthoses in the treatment of plantar fasciitis. METHODS: A pragmatic, participant-blinded, randomized trial was conducted from April 1999 to July 2001. The duration of follow-up for each participant was 12 months. One hundred and thirty-five participants with plantar fasciitis from the local community were recruited to a university-based clinic and were randomly allocated to receive a sham orthosis (soft, thin foam), a prefabricated orthosis (firm foam), or a customized orthosis (semirigid plastic). RESULTS: After 3 months of treatment, estimates of effects on pain and function favored the prefabricated and customized orthoses over the sham orthoses, although only the effects on function were statistically significant. Compared with sham orthoses, the mean pain score (scale, 0-100) was 8.7 points better for the prefabricated orthoses (95% confidence interval, -0.1 to 17.6; P = .05) and 7.4 points better for the customized orthoses (95% confidence interval, -1.4 to 16.2; P = .10). Compared with sham orthoses, the mean function score (scale, 0-100) was 8.4 points better for the prefabricated orthoses (95% confidence interval, 1.0-15.8; P = .03) and 7.5 points better for the customized orthoses (95% confidence interval, 0.3-14.7; P = .04). There were no significant effects on primary outcomes at the 12-month review. CONCLUSIONS: Foot orthoses produce small short-term benefits in function and may also produce small reductions in pain for people with plantar fasciitis, but they do not have long-term beneficial effects compared with a sham device. The customized and prefabricated orthoses used in this trial have similar effectiveness in the treatment of plantar fasciitis.
Urovitz EP, Birk-Urovitz A, Birk-Urovitz E. Endoscopic plantar fasciotomy in the treatment of chronic heel pain. Can J Surg. 2008 Aug;51(4):281-3
OBJECTIVE: To evaluate endoscopic plantar fasciotomy for the treatment of recalcitrant heel pain. METHOD: We undertook a retrospective study of the use of endoscopic plantar fasciotomy in the treatment of chronic heel pain that was unresponsive to conservative treatment. Over a 10-year period, we reviewed the charts of 55 patients with a minimum 12-month history of heel pain that failed to respond to standard nonoperative methods and had undergone the procedure described. All patients were clinically reviewed and completed a questionnaire based on the American Orthopaedic Foot and Ankle Society (AOFAS) score for ankle and hindfoot. RESULTS: The mean follow-up was 18 months. The mean preoperative AOFAS score was 66.5; the mean postoperative AOFAS score was 88.2. The mean preoperative pain score was 18.6; the mean postoperative pain score was 31.1. Complications were minimal (2 superficial wound infections). Overall, results were favourable in over 80% of patients. CONCLUSION: We conclude that endoscopic plantar fasciotomy is a reasonable option in the treatment of chronic heel pain that fails to respond to a trial of conservative treatment.
Case Studies[edit | edit source]
Young B, Walker MJ, Strunce J et al. A combined treatment approach emphasizing impairment-based manual physical therapy for plantar heal pain: a case series. JOSPT. 2004;34:725-733.
In a case series by B Young et al, they described an impairment-based physcial therapy treatment approach for 4 patients with plantar heel pain. All patients received manual therapy, consisting of posterior talocrural joint mobs and subtalar joint distraction manipulation, in combination with calf-stretching, plantar fascia stretching, and self-anterior-posterior ankle mobilization as a home program. They demonstrated complete pain relief and full return to activities with an average of 2-6 treatments per case.
Resources
[edit | edit source]
1. ↑ Lemont H, Ammirati KM, Usen N. Plantar fasciitis: a degenerative process (fasciosis) without inflammation. J Am Podiatr Med Assoc. 2003;93(3):234–7.
2. ↑ Carlson RE, Fleming LL, Hutton WC. The biomechanical relationship between the tendoachilles, plantar fascia and metatarsophalangeal joint dorsiflexion angle. Foot ankle Int / Am Orthop Foot Ankle Soc [and] Swiss Foot Ankle Soc. 2000;21(1):18–25. Level 4
3. ↑ Stecco C, Corradin M, Macchi V, et al. Plantar fascia anatomy and its relationship with Achilles tendon and paratenon. J Anat. 2013;223(August):1–12. doi:10.1111/joa.12111.
4. ↑ Gefen A, Megido-Ravid M, Itzchak Y. In vivo biomechanical behavior of the human heel pad during the stance phase of gait. J Biomech. 2001;34:1661–1665. doi:10.1016/S0021-9290(01)00143-9
5. ↑ Tweed JL, Barnes MR, Allen MJ, Campbell J a. Biomechanical consequences of total plantar fasciotomy: a review of the literature. J Am Podiatr Med Assoc. 2009;99(5):422–30.
6. ↑ Cheung, Jason Tak-Man, Kai-Nan An, and Ming Zhang. "Consequences of partial and total plantar fascia release: a finite element study." Foot & ankle international 27.2 (2006): 125-132.
7. ↑ Crary JL, Hollis JM, Manoli A. The effect of plantar fascia release on strain in the spring and long plantar ligaments. Foot ankle Int / Am Orthop Foot Ankle Soc [and] Swiss Foot Ankle Soc. 2003;24(3):245–50
8. ↑ McPoil TG, Martin RL, Cornwall MW, Wukich DK, Irrgang JJ, Godges JJ. Heel pain--plantar fasciitis: clinical practice guildelines linked to the international classification of function, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(4):A1–A18. doi:10.2519/jospt.2008.0302. Level 1A
9. ↑ Riddle DL, Pulisic M, Pidcoe P, Johnson RE. Risk factors for Plantar fasciitis: a matched case-control study. J Bone Joint Surg Am. 2003;85-A(5):872–7 Level 3B
10. ↑ Thomas JL, Christensen JC, Kravitz SR, et al. The diagnosis and treatment of heel pain: a clinical practice guideline-revision 2010. J Foot Ankle Surg. 2010;49(3 Suppl):S1–19. doi:10.1053/j.jfas.2010.01.001 Level 1A
11. ↑ Lopes AD, Hespanhol Júnior LC, Yeung SS, Costa LOP. What are the main running-related musculoskeletal injuries? A Systematic Review. Sports Med. 2012;42(10):891–905. doi:10.2165/11631170-000000000-00000. Level 2A
12. ↑ 2002 Podiatric Practice Survey. Statistical results. J Am Podiatr Med Assoc. 2003;93(1):67–86. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12533562.
13. ↑ Fabrikant JM et al; Plantar fasciitis (fasciosis) treatment outcome study: Plantar fascia thickness measured by ultrasound and correlated with patient self-reported improvement; Foot (Edinb). 2011 Mar 11. [Epub ahead of print] Level 3
14. ↑ Sutera R et al; Plantar fascia evaluation with a dedicated magnetic resonance scanner in weight-bearing position: our experience in patients with plantar fasciitis and in healthy volunteers; Radiol Med. 2010 Mar;115(2):246-60. Epub 2010 Feb 22. Level 3
15. ↑ JG Furey, Plantar fasciitis. The painfull heel syndrome, The Journal of Bone and Joint Surgery, 57:672-673 (2010)
16. ↑ Ahmed Mohamed Ahmed Othman – Ehab Mohamed Ragab, Endoscopic plantar fasciotomy versus extracorporeal shock wave therapy for treatment of chronic plantar fasciitis, Orthopaedic surgery (2009) Level 4
17. ↑ DioGiovanni BF, Nawoczenski DA, Lintal ME et al. Tissue-specific plantar fascia-stretching exercise enhance outcomes in patients with chronic heel pain. Journal of Bone and Joint Surgery. 2003;85-A:1270-1277
18. ↑ Young, Brian, et al. "A combined treatment approach emphasizing impairment-based manual physical therapy for plantar heel pain: a case series." Journal of Orthopaedic & Sports Physical Therapy 34.11 (2004): 725-733 Level 4
19. ↑ Cole C, Seto C, Gazewood J. Plantar fasciitis: evidence-based review of diagnosis and therapy. Am Fam Physician. 2005 Dec 1;72(11):2237-42. Level 3A
20. ↑ Osborne HR, Allison GT. Treatment of plantar fasciitis by LowDye taping and iontophoresis: short term results of a double blinded, randomised, placebo controlled clinical trial of dexamethasone and acetic acid. Br J Sports Med. 2006 Jun;40(6):545-9; discussion 549. Epub 2006 Feb 17. Level 1B
21. ↑ Pfeffer G, Bacchetti P, Deland J et al. Comparison of custom and prefabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot Ankle Int. 1999 Apr;20(4):214-21.
22. ↑ Landorf KB, Keenan AM, Herbert RD. Effectiveness of foot orthoses to treat plantar fasciitis: a randomized trial. Arch Intern Med. 2006 Jun 26;166(12):1305-10. Level 1B
23. ↑ Chien-Tsung Tsai et al., Effects of Short-Term Treatment with kinesiotaping for Plantar fasciitis, Journal of Musculoskeletal Pain, March 2010, Vol. 18, No. 1, Pages 71-80
24. ↑ Lori. A. Bolgla – Terry R. Malone, Plantar fasciitis and the Windlass mechanism, Journal of Athletic Training. 2004 (Jan- Mar); 39(1): 77-82
25. ↑ Alexander T. M. van de Water, Caroline M. Speksnijder, Efficacy of taping for the treatment of plantar fasciosis: a systematic review, Journal of the American Podiatric Medical Association, 2010; 1: 41-51 Level 1A
26. Goff, James D., and Robert Crawford. "Diagnosis and treatment of plantar fasciitis." American family physician 84.6 (2011): 676.
27. Fasciitis, Plantar. "Plantar Fasciitis: Diagnosis and Therapeutic Considerations." Alternative Medicine Review 10.2 (2005): 83-93.
28. Hyland, Matthew R., et al. "Randomized controlled trial of calcaneal taping, sham taping, and plantar fascia stretching for the short-term management of plantar heel pain." Journal of Orthopaedic & Sports Physical Therapy 36.6 (2006): 364-371. Level 1B
29. Riskowski, Jody L., Thomas J. Hagedorn, and Marian T. Hannan. "Measures of foot function, foot health, and foot pain: American Academy of Orthopedic Surgeons Lower Limb Outcomes Assessment: Foot and Ankle Module (AAOS‐FAM), Bristol Foot Score (BFS), Revised Foot Function Index (FFI‐R), Foot Health Status Questionnaire (FHSQ), Manchester Foot Pain and Disability Index (MFPDI), Podiatric Health Questionnaire (PHQ), and Rowan Foot Pain Assessment (ROFPAQ)." Arthritis care & research 63.S11 (2011): S229-S239.
30. Rathleff, Michael Skovdal, et al. "High‐load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12‐month follow‐up." Scandinavian journal of medicine & science in sports 25.3 (2015): e292-e300. Level 1B
31. Taping for plantar fasciitis. (n.d.) Retrieved December 08, 2016, from NISMAT: http://www.nismat.org/clinicians/athletic-training/taping-for-plantar-fasciitis
32. Acosta-Olivo C. et al.; Plantar fasciitis. A comparison of treatment with intralesional steroids versus platelet-rich plasma (PRP). A randomized, blinded study, J Am Podiatr Med Assoc.; 2016
33. Saban B. et al.; “Deep massage to posterior calf muscles in combination with neural mobilization exercises as a treatment for heel pain: a pilot randomized clinical trial.”; Manual Therapy 2014 Apr: 19; 2013 Level 2B
34. Lynn, Scott K., Ricardo A. Padilla, and Kavin KW Tsang. "Differences in static-and dynamic-balance task performance after 4 weeks of intrinsic-foot-muscle training: the short-foot exercise versus the towel-curl exercise." Journal of sport rehabilitation 21.4 (2012): 327.
35. Brian G. Donley et al.; “The Efficacy of Oral Nonsteroidal Anti-Inflammatory Medication (NSAID) in the Treatment of Plantar Fasciitis: A Randomized, Prospective, Placebo-Controlled Study”; Foot & Ankle International; 2007 Level 1B
36. Renan-Ordine, Rômulo, et al. "Effectiveness of myofascial trigger point manual therapy combined with a self-stretching protocol for the management of plantar heel pain: a randomized controlled trial." journal of orthopaedic & sports physical therapy 41.2 (2011): 43-50. (level 2)
37. Tsikopoulos K. et al.; ”Injection therapies for plantar fasciopathy (‘plantar fasciitis'): a systematic review and network meta-analysis of 22 randomised controlled trials”; BR J Sports Med.; 2016 Level 1A
38. MacAuley D, Best T, editors. Evidence-based sports medicine, Second edition. London, England: BMJ Books; 2007.
39. Sobhani S. et al. ; Epidemiology of ankle and foot overuse injuries in sports: a systematic review. Scand J Med sci Sports. 2013;23:669-686. http:/ /dx.doi.org/10.1111/j.1600-0838.2012.01509.x Level 1A
40. Hill CL. et al.; Prevalence and correlates of foot pain in a population-based study: the North West Adelaide health study. J Foot Ankle Res. 2008;1:2. http://dx.doi.org/10.1186/1757-1146-1-2
41. Lopes AD. et al.; What are the main running-related musculoskeletal injuries? A systematic review. Sports Med.2012;42:891-905. http://dx.doi.org/10.1007/BF03262301 Level 1A
42. Di Caprio F et al.; Foot and lower limb diseases in runners: assessment of risk factors. J Sports Sci Med.2010;9:587-596
43. Butterworth Pa et al.; the association between body mass index and musculoskeletal foot disorders: a systematic review. Obes Rev. 2012;13:630-642. http//dx.doi.org/10.1111/j.1467-789X.2012.00996.x (level of evidence 1)
44. Mardani-Kivi M. et al.; “Treatment Outcomes of Corticosteroid Injection and Extracorporeal Shock Wave Therapy as Two Primary Therapeutic Methods for Acute Plantar Fasciitis: A Prospective Randomized Clinical Trial”; The Journal of Foot and Ankle Surgery, Volume 54 Issue 6, pg 1047-1052; 2015
45. Celik D. et al.; “Joint mobilization and stretching exercise vs steroid injection in the treatment of plantar fasciitis: A Randomized Controlled Study”; Foot and Ankle International, Volume 37, Issue 2, pg 150-156; 2016 Level 1B
46. Martin, Robroy L., et al. "Heel pain—plantar fasciitis: revision 2014." Journal of Orthopaedic & Sports Physical Therapy (2014). Level 1A
47. Shashua, Anat, et al. "The effect of additional ankle and midfoot mobilizations on plantar fasciitis: a randomized controlled trial." journal of orthopaedic & sports physical therapy 45.4 (2015): 265-272. Level 1B
48. Thompson, John V., et al. "Diagnosis and management of plantar fasciitis." The Journal of the American Osteopathic Association 114.12 (2014): 900-901. Level 1A
49. Chen D-w, Li B, Aubeeluck A, Yang Y-f, Huang Y-g, et al. (2014) Anatomy and Biomechanical Properties of the Plantar Aponeurosis: A Cadaveric Study. PLoS ONE
50. Cutts S. et al.;Plantar fasciitis. Ann R COll Surg Engl. 2012 Nov; 94 (8):539-542. doi: 10.1308/003588412x13171221592456
51. Hafner S et al.; Proximal plantar fibroma as an etiology of recalcitrant plantar heel pain. J Foot Ankle Surg.2011;50:153-157. http://dx.doi.org/10.1053/j.fas.2010.12.016
52. Klein SE et al.; Clinical presentation and self-reported patterns of pain and function in patients with plantar heel pain. Foot ankleint. 2012;33:693-698. http://dx.doi.org.10.3113/FAI.2012.0693
53. Koumakis et al.; Heel pain in spondyloarthritis: results of a cross-sectional study of 275 patients. Clin exp rheumatol. 2012;30:487-491
54. Kulig et al.; Women with posterior tibial tendon dysfunction have diminished ankle and hip muscle performance. J Orthop Sports Phys Ther. 2011;41:687-694. http://dx.doi.org.10.2519/jospt.2011.3427
55. Miller L. et al.; Chronic plantar fasciitis is mediated by local hemodynamics: implications for emerging therapies. North American Journal of Medical Science. 2015;7(1): 1-5. doi: 10.4103/4947-2714.150080
56. Pohl MB et al.; biomechanical and anatomic factors associated with a history of plantar fasciitis in female runners. Clin J Sport Med. 2009;19:372-376
57. Ribeiro AP et al.; Rearfoot alignement and medial longitudinal arch configuartions of runners with symptomsand histories of plantar fasciitis. Clinics (Sao Paulo). 2011;66:1027-1033
58. Rio E. et al.; heel pain: a practical approach. Aust Fam Physician. 2015 Mar;44(3):96-101.
59. Tenforde As et al.; overuse injuries in high scool runners: lifetime prevalence and prevention strategies. PM R. 2011;3:125-131; quiz 131. http://dx.doi.ord/10.1016/j.pmrj.2010.09.009
60. Werner RA et al.; Risk factors for plantar fasciitis among assembly plant workers. PM R.2010;2:110-116. http://dx.doi.org/10.1016/j.pmrj.2009.11.012
61. Yi et al.; Clinical characteristics of the causes of plantar heel pain. Ann rehabil mMed. 2011;35:507-513. http://dx.doi.org/10.5535/arm.2011.35.4.507
EmbedVideo is missing a required parameter.
|
EmbedVideo is missing a required parameter.
|
Recent Related Research (from Pubmed)[edit | edit source]
Failed to load RSS feed from http://eutils.ncbi.nlm.nih.gov/entrez/eutils/erss.cgi?rss_guid=1houoX_LGC305ro2l-cEh_uDPlVE-LuIbL2pcsEP2W6Il42kL|charset=UTF-8|short|max=10: Error parsing XML for RSS
- Labovitz J et al; The Role of Hamstring Tightness in Plantar Fasciitis; Foot Ankle Spec. 2011 Mar 2. [Epub ahead of print]
Read 4 Credit[edit | edit source]
 |
Would you like to earn certification to prove your knowledge on this topic? All you need to do is pass the quiz relating to this page in the Physiopedia member area.
|
References[edit | edit source]
References will automatically be added here, see adding references tutorial.

