Back School: Difference between revisions
No edit summary |
Kim Jackson (talk | contribs) m (Text replacement - "[[Core stability" to "[[Core Stability") |
||
| (23 intermediate revisions by 7 users not shown) | |||
| Line 4: | Line 4: | ||
'''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} <br> | '''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} <br> | ||
</div> | </div> | ||
= | == Introduction == | ||
[[File:Back pain image.jpg|right|frameless]] | |||
Back schools are educational and training programs with lessons given to patients or workers by a therapist with the aim of treating or preventing [[Low Back Pain|low back pain.]] | |||
* They are a commonly used nonpharmacological intervention, especially within the [[Introduction to Occupational Health|occupational]] health setting. | |||
* Despite the use of back schools since 1969, their effectiveness in preventing or treating back pain has yet to be established unequivocally.<ref>Straube S, Harden M, Schröder H, Arendacka B, Fan X, Moore RA, Friede T. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5028160/ Back schools for the treatment of chronic low back pain: possibility of benefit but no convincing evidence after 47 years of research—systematic review and meta-analysis.] Pain. 2016 Oct;157(10):2160. Available from;https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5028160/ (last accessed 11.9.2020)</ref> | |||
The target population for back training: <ref name="Kraemer">Kraemer, J., Hasenbring, M., Kraemer, R., Taub, E., Theodoridis T., Wilke, H.J., 'Intervertebral disk diseases: causes, diagnosis, treatment and prophylaxis', Thieme, 2009, p. 321-327</ref> | The target population for back training: <ref name="Kraemer">Kraemer, J., Hasenbring, M., Kraemer, R., Taub, E., Theodoridis T., Wilke, H.J., 'Intervertebral disk diseases: causes, diagnosis, treatment and prophylaxis', Thieme, 2009, p. 321-327</ref> | ||
*Patients who have never had low back pain (primary intervention). | *Patients who have never had low back pain (primary intervention). | ||
*Back school | *Back school ( secondary prevention)- eg episodes of acute or [[Chronic Low Back Pain|chronic low back pain]]; recurrenceof a specific low back pain; post-operative spinal surgery patients. | ||
*People with low back pain that can be linked to the clinically relevant anatomy. | |||
The intensity and content of back schools differ. | |||
The | |||
eg. Contents Swedish Back School ( four 45-min sessions during a 2-week period) | |||
# Anatomy and causes of LBP and [[Psoas Major|psoas]] position | |||
# Function of the [[Muscle Biomechanics|muscles]] and [[Therapeutic Exercise|exercise]]<nowiki/>s | |||
# [[Work-Related Musculoskeletal Injuries and Prevention|Ergonomics]] | |||
# Advice on [[Physical Activity|physical activity]] | |||
# One individual session of [[Aquatherapy|pool exercises]] under the supervision of a physiotherapist and an analysis of the working condition by a physiotherapist<ref name=":0">Keijsers JF, Steenbakkers MW, Gerards FM, Meertens RM. [https://onlinelibrary.wiley.com/doi/pdf/10.1002/art.1790030409 The efficacy of the back school: An analysis of the literature. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology.] 1990 Dec;3(4):210-5.Available from:https://onlinelibrary.wiley.com/doi/pdf/10.1002/art.1790030409 (last accessed 11.9.2020)</ref>. | |||
= | == Typical Content == | ||
The Swedish Back School was developed by Zachrisson Forsell and consists of four 45-min, mainly audiovisual, lessons under the supervision of a physiotherapist. | |||
'''First session''' - different aspects of back disorders are discussed. | |||
* The patients are given full details of the anatomy and function of the back. | |||
* Various methods of treatment are discussed and the psoas position is taught. | |||
* The entire course takes place with the patients in this position instead of in the seated position. | |||
[[File:Computer-posture.jpg|right|frameless|564x564px]] | |||
'''Second session''' - the mechanical strain of different positions and during different movements is discussed. | |||
* The function of the muscles and their influence on the back are demonstrated. | |||
* The patients are instructed in isometric [[Abdominal Muscles|abdominal muscle]] exercises and encouraged to continue these exercises every day. | |||
* [[Back Education Program|Back muscle exercises]] are discussed and the patients are told that these exercises expose the back to increased strain, with a risk of aggravation of the symptoms. | |||
'''Third session''' - consists of practical application of the previously acquired theoretical knowledge. | |||
* The patients are asked to describe their own work situation and the group endeavours to arrive at a suitable solution for each individual. | |||
'''Fourth session''' - consists mainly of encouraging the patients to increase their level of physical activity during leisure hours in spite of their back disorder. | |||
* A written summary of the principal contents of the Back School is provided. | |||
* Patients attending the back school are also offered one session of pool exercises under the supervision of a physiotherapist.<br> | |||
== Physical Therapy Management == | |||
Goals of patients who attend a back school: | Goals of patients who attend a back school: | ||
*Functional recovery: protect the spinal structures in daily activities and in the occupational setting | *Functional recovery: protect the spinal structures in daily activities and in the occupational setting | ||
*Reduce symptoms (pain) | *Reduce symptoms (pain) | ||
* | *Increasing tissue repair | ||
* | *Decrease kinesiophobia | ||
To achieve these goals, the back school consists of three parts: | To achieve these goals, the back school consists of three parts: | ||
# | #Education about the anatomy and function of the spine, spinal biomechanics, physiopathology of frequent back disorders, epidemiology… Nowadays, this part of back school (giving information) is limited as compared to the back school in 1969 <ref name="Kraemer" />. An example part of education session is eg The biomechanical principles: Functional load / compression on the nucleus pulposus results in a deformation without changing the volume of the nucleus. When a persistent compression is applied to the anulus fibrosus, it will release water. The height of the disc decreases, so there is more compression on the nucleus pulposus. The disc needs compression to maintain the metabolic activity of the disc, osmotic system of the disc Lumbosacral Biomechanics. But when the compression is too high, the intradiscular pressure increases and can develop in low back pain. Some body postures and movements increase this intradiscal pressure.<ref name="Kraemer" /> | ||
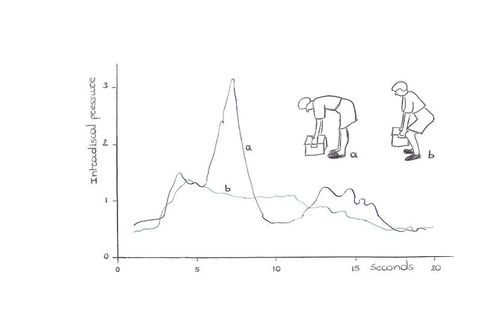
# | #[[File:Biomechanical 2.jpg|right|frameless|500x500px]]Training for posture in standing, lifting, bending, lying, sitting etc. Differs for the occupational settings:<ref name="Kraemer" /> eg Banker. A banker sits the whole day, so it’s important he’s sitting in a correct way: When he bends forward while sitting, the intradiscal pressure is supposed to be twice as high as while standing. The correct way of sitting: both feet supported on the ground, situated below the knees at waist level. The waist is situated a little higher than the knees and leaning with a straight back against the backrest. It’s also important his worksheet is situated at a correct height; Shelf packer-the intradiscal pressure by lifting a box taught see graph R you can see the intradiscal pressure by two types of lifting. It’s by the principal of the lever. As the load and load arm are smaller, the force required to keep the lever in balance is smaller too.<ref name="Kraemer" /> <br> | ||
#Active protection of the spine by | #Active protection of the spine by active exercises<ref name="Kraemer" /><ref name="Garcia">Garcia, A., Gondo, F., Costa, R., Cyrillo, F., Silva, T., Costa, L. CM, Costa, L. OP, 'Effectiveness of the back school and mckenzie techniques in patients with chronic non-specific low back pain: a protocol of a randomised controlled trial', BMC Musculoskeletal Disorders, 2011, nr. 12</ref>eg Stretching of the lower limbs muscles; Stretching of the erector spinae muscles; Kinaesthetic training (move pelvis making a front and back pelvic inclination at a comfortable range); Strengthening of the [[Core Stability|core]] (stabilizing function).<ref name="Kraemer" /><ref name="Heymans">Heymans, M., Van Tulder, M., Esmail, R., Bombardier, C., Koes, B., 'Back schools for nonspecific low back pain', Spine, 2005, Vol. 30, nr. 19, p. 2153-2163 (Level of evidence 1A)</ref> | ||
== Key Evidence == | |||
< | From the Cochrane review 3.8.2017 | ||
= Key Evidence = | |||
"Due to the low- to very low-quality of the evidence for all treatment comparisons, outcomes, and follow-up periods investigated, it is uncertain if Back School is effective for <abbr>chronic</abbr> low back pain. Although the quality of the evidence was mostly very low, the results showed no difference or a trivial effect in favour of Back School. There are myriad potential variants on the Back School approach regarding the employment of different exercises and educational methods. While current evidence does not warrant their use, future variants on Back School may have different effects and will need to be studied in future <abbr>RCTs</abbr> and reviews"<ref>Parreira P, Heymans MW, van Tulder MW, Esmail R, Koes BW, Poquet N, Lin CW, Maher CG. [https://www.cochrane.org/CD011674/BACK_back-school-treatment-chronic-low-back-pain Back Schools for chronic non‐specific low back pain.] Cochrane Database of Systematic Reviews. 2017(8).Available from:https://www.cochrane.org/CD011674/BACK_back-school-treatment-chronic-low-back-pain (last accessed 11.9.2020)</ref> | |||
== References == | |||
<br> | <references /> <br> | ||
[[Category:Health_Promotion]] | |||
[[Category:Lumbar Spine]] | |||
[[Category:Lumbar Spine - Interventions]] | |||
Latest revision as of 16:23, 13 November 2021
Original Editor - Lien Hennebel
Top Contributors - Sheik Abdul Khadir, Lien Hennebel, Lucinda hampton, Admin, WikiSysop, Kim Jackson, 127.0.0.1 and Rachael Lowe
Introduction[edit | edit source]

Back schools are educational and training programs with lessons given to patients or workers by a therapist with the aim of treating or preventing low back pain.
- They are a commonly used nonpharmacological intervention, especially within the occupational health setting.
- Despite the use of back schools since 1969, their effectiveness in preventing or treating back pain has yet to be established unequivocally.[1]
The target population for back training: [2]
- Patients who have never had low back pain (primary intervention).
- Back school ( secondary prevention)- eg episodes of acute or chronic low back pain; recurrenceof a specific low back pain; post-operative spinal surgery patients.
- People with low back pain that can be linked to the clinically relevant anatomy.
The intensity and content of back schools differ.
eg. Contents Swedish Back School ( four 45-min sessions during a 2-week period)
- Anatomy and causes of LBP and psoas position
- Function of the muscles and exercises
- Ergonomics
- Advice on physical activity
- One individual session of pool exercises under the supervision of a physiotherapist and an analysis of the working condition by a physiotherapist[3].
Typical Content[edit | edit source]
The Swedish Back School was developed by Zachrisson Forsell and consists of four 45-min, mainly audiovisual, lessons under the supervision of a physiotherapist.
First session - different aspects of back disorders are discussed.
- The patients are given full details of the anatomy and function of the back.
- Various methods of treatment are discussed and the psoas position is taught.
- The entire course takes place with the patients in this position instead of in the seated position.

Second session - the mechanical strain of different positions and during different movements is discussed.
- The function of the muscles and their influence on the back are demonstrated.
- The patients are instructed in isometric abdominal muscle exercises and encouraged to continue these exercises every day.
- Back muscle exercises are discussed and the patients are told that these exercises expose the back to increased strain, with a risk of aggravation of the symptoms.
Third session - consists of practical application of the previously acquired theoretical knowledge.
- The patients are asked to describe their own work situation and the group endeavours to arrive at a suitable solution for each individual.
Fourth session - consists mainly of encouraging the patients to increase their level of physical activity during leisure hours in spite of their back disorder.
- A written summary of the principal contents of the Back School is provided.
- Patients attending the back school are also offered one session of pool exercises under the supervision of a physiotherapist.
Physical Therapy Management[edit | edit source]
Goals of patients who attend a back school:
- Functional recovery: protect the spinal structures in daily activities and in the occupational setting
- Reduce symptoms (pain)
- Increasing tissue repair
- Decrease kinesiophobia
To achieve these goals, the back school consists of three parts:
- Education about the anatomy and function of the spine, spinal biomechanics, physiopathology of frequent back disorders, epidemiology… Nowadays, this part of back school (giving information) is limited as compared to the back school in 1969 [2]. An example part of education session is eg The biomechanical principles: Functional load / compression on the nucleus pulposus results in a deformation without changing the volume of the nucleus. When a persistent compression is applied to the anulus fibrosus, it will release water. The height of the disc decreases, so there is more compression on the nucleus pulposus. The disc needs compression to maintain the metabolic activity of the disc, osmotic system of the disc Lumbosacral Biomechanics. But when the compression is too high, the intradiscular pressure increases and can develop in low back pain. Some body postures and movements increase this intradiscal pressure.[2]
- Training for posture in standing, lifting, bending, lying, sitting etc. Differs for the occupational settings:[2] eg Banker. A banker sits the whole day, so it’s important he’s sitting in a correct way: When he bends forward while sitting, the intradiscal pressure is supposed to be twice as high as while standing. The correct way of sitting: both feet supported on the ground, situated below the knees at waist level. The waist is situated a little higher than the knees and leaning with a straight back against the backrest. It’s also important his worksheet is situated at a correct height; Shelf packer-the intradiscal pressure by lifting a box taught see graph R you can see the intradiscal pressure by two types of lifting. It’s by the principal of the lever. As the load and load arm are smaller, the force required to keep the lever in balance is smaller too.[2]
- Active protection of the spine by active exercises[2][4]eg Stretching of the lower limbs muscles; Stretching of the erector spinae muscles; Kinaesthetic training (move pelvis making a front and back pelvic inclination at a comfortable range); Strengthening of the core (stabilizing function).[2][5]

Key Evidence[edit | edit source]
From the Cochrane review 3.8.2017
"Due to the low- to very low-quality of the evidence for all treatment comparisons, outcomes, and follow-up periods investigated, it is uncertain if Back School is effective for chronic low back pain. Although the quality of the evidence was mostly very low, the results showed no difference or a trivial effect in favour of Back School. There are myriad potential variants on the Back School approach regarding the employment of different exercises and educational methods. While current evidence does not warrant their use, future variants on Back School may have different effects and will need to be studied in future RCTs and reviews"[6]
References[edit | edit source]
- ↑ Straube S, Harden M, Schröder H, Arendacka B, Fan X, Moore RA, Friede T. Back schools for the treatment of chronic low back pain: possibility of benefit but no convincing evidence after 47 years of research—systematic review and meta-analysis. Pain. 2016 Oct;157(10):2160. Available from;https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5028160/ (last accessed 11.9.2020)
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 Kraemer, J., Hasenbring, M., Kraemer, R., Taub, E., Theodoridis T., Wilke, H.J., 'Intervertebral disk diseases: causes, diagnosis, treatment and prophylaxis', Thieme, 2009, p. 321-327
- ↑ Keijsers JF, Steenbakkers MW, Gerards FM, Meertens RM. The efficacy of the back school: An analysis of the literature. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology. 1990 Dec;3(4):210-5.Available from:https://onlinelibrary.wiley.com/doi/pdf/10.1002/art.1790030409 (last accessed 11.9.2020)
- ↑ Garcia, A., Gondo, F., Costa, R., Cyrillo, F., Silva, T., Costa, L. CM, Costa, L. OP, 'Effectiveness of the back school and mckenzie techniques in patients with chronic non-specific low back pain: a protocol of a randomised controlled trial', BMC Musculoskeletal Disorders, 2011, nr. 12
- ↑ Heymans, M., Van Tulder, M., Esmail, R., Bombardier, C., Koes, B., 'Back schools for nonspecific low back pain', Spine, 2005, Vol. 30, nr. 19, p. 2153-2163 (Level of evidence 1A)
- ↑ Parreira P, Heymans MW, van Tulder MW, Esmail R, Koes BW, Poquet N, Lin CW, Maher CG. Back Schools for chronic non‐specific low back pain. Cochrane Database of Systematic Reviews. 2017(8).Available from:https://www.cochrane.org/CD011674/BACK_back-school-treatment-chronic-low-back-pain (last accessed 11.9.2020)

