Bursitis: Difference between revisions
Aarti Sareen (talk | contribs) No edit summary |
Aarti Sareen (talk | contribs) No edit summary |
||
| Line 5: | Line 5: | ||
Bursitis is the inflammation of a bursa. <br> | Bursitis is the inflammation of a bursa. <br> | ||
== Comman sites<br> == | |||
Subacromial bursitis<br> Olecranon bursitis - students elbow<br> | |||
Prepatellar bursitis - housemaid's knee"<br> Infrapatellar bursitis - clergyman's knee"<br> Trochanteric bursitis of hip<br> Achilles bursitis<br> Retrocalcaneal bursitis<br> Ischial bursitis - weaver's bottom"<br> Iliopsoas bursitis<br> Pesanserine bursitis<br><br> | |||
== Clinically Relevant Anatomy<br> == | == Clinically Relevant Anatomy<br> == | ||
| Line 39: | Line 45: | ||
In most cases bursitis can be diagnosed by physically examining the patient. | In most cases bursitis can be diagnosed by physically examining the patient. | ||
<u></u><u><span | <u></u><u><span style="display: none;" id="1308682643946S"> </span>Inspection</u>: | ||
*Redness and warmth can be signs of bursitis, but these symptoms are harder to spot when treating a Bursa that is not located superficial under the skin. | *Redness and warmth can be signs of bursitis, but these symptoms are harder to spot when treating a Bursa that is not located superficial under the skin. | ||
| Line 73: | Line 79: | ||
*When improvement is noticeable, <u>gradual</u> increase in exercise and activities is recommended. | *When improvement is noticeable, <u>gradual</u> increase in exercise and activities is recommended. | ||
<span style="display: none; | <span id="1308683459810S" style="display: none;"> </span>''Note'': Resting the affected joint does not mean immobilizing it, this could hold a risk towards adhesive capsulitis (especially in the shoulder). | ||
<u>Bursitis due to infection</u> ('''= septic bursitis'''): | <u>Bursitis due to infection</u> ('''= septic bursitis'''): | ||
| Line 83: | Line 89: | ||
<br> | <br> | ||
<span style="display: none; | <span id="1308683600457S" style="display: none;"> </span> ''Note: ''When measures mentioned above are inadequate surgical interventions may be necessary<br>in case of following factors: | ||
*surgical removal of the bursa is recommended in case of tuberculous bursitis | *surgical removal of the bursa is recommended in case of tuberculous bursitis | ||
| Line 116: | Line 122: | ||
6. Woodley S.J., Nicholson H.D., Livingstone V., Doyle T.C., Meikle G.R., Macintosh J.E., Mercer S.R. Lateral Hip Pain: Findings From<br>7. Magnetic Resonance Imaging and Clinical Examination. Journal of orthopaedic & sports physical therapy, Vol 38, No. 6, June 2008, pp 313 – 328<br>8. Paluska S.A., An overview of Hip Injuries in Running. Sports Med 2005; 35, pp 991 – 1014<br><br> | 6. Woodley S.J., Nicholson H.D., Livingstone V., Doyle T.C., Meikle G.R., Macintosh J.E., Mercer S.R. Lateral Hip Pain: Findings From<br>7. Magnetic Resonance Imaging and Clinical Examination. Journal of orthopaedic & sports physical therapy, Vol 38, No. 6, June 2008, pp 313 – 328<br>8. Paluska S.A., An overview of Hip Injuries in Running. Sports Med 2005; 35, pp 991 – 1014<br><br> | ||
{| cellspacing="5" cellpadding="2 | {| cellspacing="5" cellpadding="2" style="margin: 15px 0pt 0pt; border: 1px solid rgb(163, 177, 191); width: 100%; color: rgb(0, 0, 0); vertical-align: top; background-color: rgb(227, 228, 250);" class="FCK__ShowTableBorders" | ||
|- | |- | ||
| The content on or accessible through Physiopedia is for informational purposes only. Physiopedia is not a substitute for professional advice or expert medical services from a qualified healthcare provider. [[Physiopedia:Terms of Service|Read more]]. | | The content on or accessible through Physiopedia is for informational purposes only. Physiopedia is not a substitute for professional advice or expert medical services from a qualified healthcare provider. [[Physiopedia:Terms of Service|Read more]]. | ||
|} | |} | ||
Revision as of 20:41, 5 November 2013
Definition/Description[edit | edit source]
Bursitis is the inflammation of a bursa.
Comman sites
[edit | edit source]
Subacromial bursitis
Olecranon bursitis - students elbow
Prepatellar bursitis - housemaid's knee"
Infrapatellar bursitis - clergyman's knee"
Trochanteric bursitis of hip
Achilles bursitis
Retrocalcaneal bursitis
Ischial bursitis - weaver's bottom"
Iliopsoas bursitis
Pesanserine bursitis
Clinically Relevant Anatomy
[edit | edit source]
A Bursa appears at a junction of a tendon on the bone. A bura is filled with a thin layer of synovial fluid. It protects and brakes the shocks of the joint. The structures nearby the bursa can move with minimal friction due to irritation. They have different measures and are mostly flattened.


Mechanism of Injury / Pathological Process
[edit | edit source]
When a Bursa gets inflamed, it swells, develops friction and starts irritating the muscle tendon it is supposed to protect. This way the bursa and muscle tendon get more and more irritated.
These issues lead to bursitis and tendinitis.
Bellow is a summary of causes for bursitis, with the example for the olecranon bursa.
- Overuse of the joint: for example vacuuming for hours on end
- Repetitive strain: for example picking up and lifting heavy loads
- Trauma: by falling on your elbow or bumping it against something
- Pressure: leaning on the elbow at a desk is a common cause of bursitis among students
- Bacterial infection: from an unattended wound (this is called septic bursitis)
- Other inflammatory diseases: Gout for instance : the gout crystals can form in the bursa and cause the inflammation.
Epidemiology/Etiology[edit | edit source]
Bursitis may occur:
- Mainly by constant friction, thumping or pressure
- The inflammation of the bursa frequently appears in combination with tendinitis
- By an overuse injury or a trauma, especially when pulling and pushing heavy items
- After a forced period of rest
- There also can be an underlying rheumatic condition
- Diabetes, osteoarthritis and disability of the thyroid gland can be associated to bursitis
Clinical Presentation[edit | edit source]
add text here relating to the clinical presentation of the condition
Diagnostic Procedures[edit | edit source]
In most cases bursitis can be diagnosed by physically examining the patient.
Inspection:
- Redness and warmth can be signs of bursitis, but these symptoms are harder to spot when treating a Bursa that is not located superficial under the skin.
- Local tenderness or stiffness.
- Swelling can occur when inflammation gets worse.
X-ray:
- Can rule out arthritis and bone deformities
- Can sometimes confirm the presence of following substances inside the bursa (By which it become visible in X ray)
- Gout crystals
- Calcifications: When the condition is chronic or recurrent. -
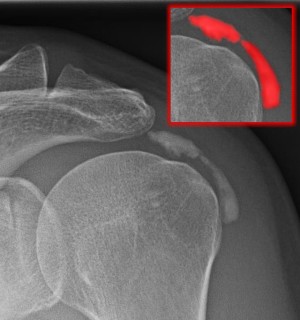

Calcified bursitis in shoulder X ray
Bursa fluid punction:
- Can rule out infections.
Outcome Measures[edit | edit source]
add links to outcome measures here (see Outcome Measures Database)
Management / Interventions[1][2]
[edit | edit source]
Bursitis due to movement/activity (without infection):
- Rest the affected joint/ bursa
- Ice packages
- NSAID’s ( non steroid anti inflammatory drugs)
- Injections with steroid agents
- When improvement is noticeable, gradual increase in exercise and activities is recommended.
Note: Resting the affected joint does not mean immobilizing it, this could hold a risk towards adhesive capsulitis (especially in the shoulder).
Bursitis due to infection (= septic bursitis):
- Antibiotics
- Aspiration of the infected bursa fluid with the use of a sterile needle should be repeated approximately every 3 days
- Never inject with steroids!
Note: When measures mentioned above are inadequate surgical interventions may be necessary
in case of following factors:
- surgical removal of the bursa is recommended in case of tuberculous bursitis
- Surgical incision and drainage is recommended in case of :
- Failure of adequately aspirating by needle
- Bursa site inaccessible to multiple needle aspirations
- Forming of abscess or necrosis
Differential Diagnosis
[edit | edit source]
add text here relating to the differential diagnosis of this condition
Key Evidence[edit | edit source]
add text here relating to key evidence with regards to any of the above headings
Resources
[edit | edit source]
http://www.medicinenet.com/bursitis/article.htm
http://emedicine.medscape.com/article/822693-treatment
http://www.reumaliga.be/vrliburs.htm
http://www.medicinenet.com/bursitis/article.htm
http://www.associatie-orthopedie-lier.be/Generic/servlet/Main.html;jsessionid=914EE2C36D10FED19214703AB3947179?p_pageid=102194
http://www.orthopedieherentals.be/index.php?page=olecranon-bursitis
http://www.reumanet.be/aandoeningen/bursitis.html
Case Studies[edit | edit source]
add links to case studies here (case studies should be added on new pages using the case study template)
References[edit | edit source]
- ↑ Ce´dric Perez1 ET AL. Infectious olecranon and patellar bursitis: short-course adjuvant antibiotic therapy is not a risk factor for recurrence in adult hospitalized patients: Journal of Antimicrob Chemotherapy 2010; 65: 1008–1014 (Evidence level B)
- ↑ S. P. Cohen ET AL. Corticosteroid injections for trochanteric bursitis: is fluoroscopy necessary? A pilot study. : British Journal of Anaesthesia 94 (1): 100–6 (2005)(Evidence level C)
3. Van de Perre S., Vanwambeke K., Vanhoenacker F.M., De Schepper A.M., Posttraumatic iliopsoas bursitis, JBR-BTR, 2005, 88:154-155
4. Johnston C.A.M., Wiley J.P., Lindsay D.M., Wisemand D.A., Iliopsoas bursitis and tendinitis (a review), Sports Med, april 1998; 25 (4): 271 – 283 (Level of evidence: A1)
5. Ombregt L., Bisschop P., ter Veer H.J., Van de Velde T., A System of Orthopaedic Medicine. 1999.
6. Woodley S.J., Nicholson H.D., Livingstone V., Doyle T.C., Meikle G.R., Macintosh J.E., Mercer S.R. Lateral Hip Pain: Findings From
7. Magnetic Resonance Imaging and Clinical Examination. Journal of orthopaedic & sports physical therapy, Vol 38, No. 6, June 2008, pp 313 – 328
8. Paluska S.A., An overview of Hip Injuries in Running. Sports Med 2005; 35, pp 991 – 1014
| The content on or accessible through Physiopedia is for informational purposes only. Physiopedia is not a substitute for professional advice or expert medical services from a qualified healthcare provider. Read more. |

