Femoral Neck Hip Fracture
Original Editor - Delmoitie Giovanni
Top Contributors - Delmoitie Giovanni, Lucinda hampton, Simisola Ajeyalemi, Jessie Tourwe, Joyce De Gelas, Kim Jackson, Admin, Tolulope Adeniji, Debontridder Jordy, Aminat Abolade, Sara Evenepoel, Yarne Leuckx, Vidya Acharya, Annelies Beckers, Elien Lebuf, Karen Wilson, Claire Knott and Lauren Lopez
Introduction[edit | edit source]
.jpeg)
Hip Fracture (Image R: hip fracture xray):
- Vernacular term for fracture of the femoral neck, typically resulting from a fall in an old person with osteoporosis; more common in women; requires surgical repair with internal fixation and can lead to prolonged or permanent loss of mobility and shortened life span[1].
- Common injury sustained by older patients who are both more likely to have unsteadiness of gait and reduced bone mineral density, predisposing to fracture.
- The biggest risk factors for a hip fracture are osteoporosis and cognitive impairment.[2][3]
- About one-third of elderly people living independently fall every year, with 10% of these falls resulting in a hip fracture.[4]
- A serious injury that occurs mostly in elderly people and complications can be life-threatening.[5][3]
- In younger patients femur fractures are the result of a high energy trauma, such as a motor accident, gunshot wound, or jump/fall from a height.[3]
- High mortality, long-term disability and huge socio-economic burden are the main consequences of a hip fracture.
Clinically Relevant Anatomy[edit | edit source]

The hip joint is a
- Ball and socket joint, formed by the head of the femur and the acetabulum of the pelvis.
- Very sturdy joint, due to the tight fitting of the bones and the strong surrounding ligaments and muscles.
The femur connects at the acetabulum of the pelvis and projects laterally before angling medially and inferiorly to form the knee.
A hip fracture occurs just below the head of femur (HOF) ie the region of the femur called the femoral neck. A femoral neck fracture disconnects the HOF from the rest of the femur,
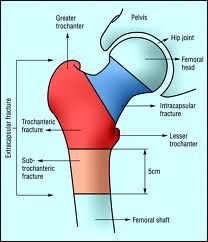
Hip fractures can be classified into intracapsular (femoral neck) fractures and extracapsular fractures. The intracapsular fractures are contained within the hip capsule itself. Those fractures are subcapital neck fracture and transcervical neck fracture. The extracapsular fractures are intertrochantericic and subtrochanteric fracture. You also have a greater and lesser trochantefracturees[6] (figure1)
Click Hip Anatomy for more details
Epidemiology[edit | edit source]
Approximately 1.6 million hip fractures occur worldwide each year, by 2050 this number could reach between 4.5 million and 6.3 million.
- Between 1990 and 2000, there was nearly a 25% increase in hip fractures worldwide. The peak number of hip fractures occurred at 75-79 years of age for both sexes.
- Nearly 75% of all hip fractures occur in women.
- Men account for 25% of hip fractures occurring in the over 50 population.
- Hip fractures are invariably associated with chronic pain, reduced mobility, disability, and an increasing degree of dependence.
- After sustaining a hip fracture 10-20% of formerly community dwelling patients require long term nursing care, with the rate of nursing home admission rising with age.
- In white women, the lifetime risk of hip fracture is 1 in 6.
- A 50 year old woman has a 2.8% risk of death related to hip fracture during her remaining lifetime.
- 5-10% of patients experience a recurrent hip fracture, with the mean interval between the first and second fracture being 3.3 years .
- Up to 20% of patients die in the first year following hip fractures, mostly due to pre-existing medical conditions. Less than half those who survive the hip fracture regain their previous level of function[7]

Classification of Hip Fractures[edit | edit source]
Hip fractures: Classified into intracapsular and extracapsular fractures[8]
Intracapsular fractures (femoral neck fractures): Occurs within the hip capsule; accounts for 45% of all acute hip fractures in the elderly[9]; susceptible to malunion/avascular necrosis of the HOF because of the limited blood supply to the area.

Intracapsular fractures are further classified as nondisplaced or displaced based on radiographic findings[10]
- Type 1: undisplaced and incomplete fracture
- Type 2: undisplaced complete fracture
- Type 3: complete fracture but incompletely displaced
- Type 4: complete fracture and completely displaced
Extracapsular fractures: intertrochanteric fracture or subtronchanteric fracture.
- Intertrochanteric fracture: occurs between the greater and the lesser trochanter[8]; intertrochanteric region has a good blood supply, avascular necrosis or nonunion is rare.
- Subtronchanteric fracture: occurs below the lesser trochanter, approximately 2.5 inches below
Etiology[edit | edit source]
Most commonly:
- Falls in the elderly: in elderly patients, the mechanism of injury various from falls directly onto the hip to a twisting mechanism in which the patient’s foot is planted and the body rotates. There is generally deficient elastic resistance in the fractured bone[2].
- More than 50% of hip fracture patients have osteoporosis, and nearly all are osteopenia[11]
- The majority of fragility hip fractures occurred inside the home[12]
- Significant trauma (e.g. motor vehicle collisions) in younger patients
- About 3% of hip fractures are related to localized bone weakness at the fracture site, secondary to tumor, followed by bone cysts, or Paget’s disease.
Risk factors[edit | edit source]
Risk factors for hip fracture include[13][14]:
- Gender: prevalent in women; postmenopausal twice as likely as premenopausal to have hip fracture[15]
- Reduced Bone density[16]
- Fall[17]
- Medications: Some medications can cause a decrease in bone density like cortisone.
- Nutrition: It is well known that calcium and vitamin D increase bone mass, so a lack of it can cause several fractures, including hip fractures.
- Age: the older you get, the higher the risk is for hip fractures. 90% of these fractures occur in persons over 70 years old.
- Alcohol and tobacco: These products can reduce the bone mass, causing a higher risk to have a hip fracture
- Medical problems: Endocrine disorders can cause fragility of the bones
- Physical inactivity: Physical activity is very important for the muscle mass and the bone mass
- Stroke disease increases risk factor for falls which can cause a hip fracture.
- Parkinson’s disease increases risk factor for falls which can cause a hip fracture.
Characteristics/Clinical Presentation[edit | edit source]
- Dull ache in the groin and/or hip region[11]
- Inability to put weight on the injured leg causing immobility right after the fall[18]
- Shorter leg on the side of the injured hip
- External rotation of the injured leg[18]
- Stiffness, bruising and swelling in and around the hip
Diagnostic Procedures[edit | edit source]
The diagnosis of a hip fracture is established based on patient history, physical examination, and radiography.[18]
- Plain radiographs (sensitivity 93-98%) is the first-line investigation for suspected NOF fractures.
- In patients with a suspected occult NOF fracture, MRI (sensitivity 99-100%) is recommended by many institutions as the second-line test if available within 24 hours, with CT or nuclear medicine bone scan third-line[2]
Outcome Measures[edit | edit source]
- Functional Independence Measure
- Berg Balance Scale
- Timed Up and Go Test (TUG)
- Patient Specific Functional Scale
- Falls Risk Assessment Tool
Treatment and Prognosis[edit | edit source]

The management of hip fracture is usually a combination of surgery and rehabilitation.
- Also depends on the location of the fracture and whether it is displaced.
- In comparison to conservative management (bed rest and traction), operative management results in a reduced length of hospital stay and improved rehabilitation.[19]
- Significant complications such as avascular necrosis and non-union are very common without surgical intervention.
- The treatment options include non-operative management, internal fixation or prosthetic replacement.
- Internal fixation can be performed with multiple pins, intramedullary hip screw (IHMS), crossed screw-nails or compression with a dynamic screw and plate.
- Replacing the femoral head is achieved with either hemiarthroplasty and total hip arthroplasty.
The high morbidity and mortality associated with hip and pelvic fractures after trauma has been well documented.
- Prognosis is varied but is complicated by advanced age, as hip fractures increase the risk of death and major morbidity in the elderly.
- Surgery <48 hours after admission may be associated with lower morbidity and may decrease hospital stay.[20][21].[22][23]
- The risk of avascular necrosis (AVN) depends on the type of fracture: Transphyseal: ~90% risk of AVN; Subcapital: ~50% risk of AVN; Basicervical/transcervical: ~25% risk of AVN; Intertrochanteric: ~10% risk of AVN[2]
Physical Examination[edit | edit source]
On physical examination, findings on the patient with a hip fracture may include the following:
- limited and painful hip range of motion, especially in internal rotation.
- the injured leg is shortened, externally rotated, and abducted in the supine position
- Pain is noted upon attempted passive hip motion.
- Ecchymosis may or may not be present.
- An antalgic gait pattern may be present.
- Tenderness to palpation around the inguinal area, over the femoral neck. This area may also be swollen.
- Increased pain on the extremes of hip rotation, an abduction lurch, and an inability to stand on the involved leg
For more on Hip examination, click www.physio-pedia.com/Hip_Examination
Physical Therapy Management[edit | edit source]
The patient training begins the day after surgery from a sitting position, with abducted hip during transfer from bed to chair.[24]
- On the second and third post-operative day the patient can start with walking between parallel bars, and later on, they can walk with a walker or a cane. A warming up on a stationary bicycle for 10 to 15 minutes is recommended.[25]
- Progressive weight-bearing as tolerated till full weight-bearing should start soon after surgery according to general physical status. Range of motion exercises should also be included.
- When internal fixation is performed, partial weight-bearing is recommended for a period of 8–10 weeks (according to the radiological evaluation of fracture healing), and after 3 months full weight-bearing should be allowed.
- The patient can also begin strengthening exercises based on the surgeon's orders (typically six weeks post-op).
- Patients should also undergo balance and proprioceptive rehab and these abilities are quickly lost with inactivity.
Prolonged bed rest can increase the risk of pressure sores, atelectasis, pneumonia, deconditioning, and thromboembolic complications. Weight-bearing immediately after hip fracture surgery is safe in most patients.[26] Complications following hip surgery involve blood clots, pneumonia, wound infections, and more, all of which can be reduced with activity[27]
Key component of rehabilitation is education and prevention. Home safety to prevent falls, regular moderate exercise can slow bone loss and maintain muscle strength, also improve balance and coordination.
There are some important rules postoperative:
- internal rotation from hip flexion is very stressful for the joint
- impact activities should be avoided for six weeks postoperative
- depending on the surgical procedure is unloaded or partially loaded mobilize postoperatively crucial to the joint
- Avoid straight leg raise for 4 weeks postoperatively to not provoke irritation of the nerve
- Cardiovascular training is important
Weight-bearing exercises are very important for mobility, balance, activities of daily living and quality of life[28], examples: stepping in different directions, standing up and sitting down, tapping the foot and stepping onto and off a block.

For patients who underwent a prosthetic replacement have to avoid for approximately 12 weeks:
- Hip flexion greater than 70–90°
- External rotation of the leg
- Adduction of the leg past midline
- Should not bend forward from the waist more than 90
Rehabilitation program components[29]:
- Hip extension (theraband and manual exercise)
- Heel raises onto toes (theraband and manual exercise)
- Resisted rowing (double arm lifting) (theraband and manual exercise)
- Standing diagonal reach (theraband and manual exercise)
- Modified get up and go (theraband and manual exercise)
- Overhead arm extensions (theraband and manual exercise)
- Repeated chair stands (vest and manual exercise)
- Lunges - forward and back (vest and manual exercise)
- Stepping up and down step (vest, manual exercise and plyometric step)
- Calf raises - both legs and one leg (manual exercise)
Importance or rehabilitation/home exercise program:
- Moderate to large improvements in physical performance and quality of life was found in patients who had a 10- week home-based progressive resistance exercise program[30]
- A meta-analyses, showed that balance training within 6 months improves person with hip fracture physical functioning, gait, lower limb strength, performance task, and activity of daily living.[31]
- Among patients who had completed standard rehabilitation after hip fracture, the use of a home-based functionally oriented exercise program resulted in modest improvement in physical function at 6 months after randomization.[32]
Clinical Bottom Line[edit | edit source]
The number of hip fractures worldwide will increase up to 7-21 million incidences each year in 2050.[33] Mortality associated with a hip fracture is about 5-10% after one month. One year after fracture, about a third of patients will have died, compared with an expected annual mortality of about 10% in this age group.[33]Thus, only a third of the deaths are directly attributable to the hip fracture itself, but patients and relatives often think that the fracture has played a crucial part in the final illness. More than 10% of survivors will be unable to return to their previous residence. Most of the remainder will have some residual pain or disability. Most people who sustain the injury require surgery followed by a period of rehabilitation. Treatment is generally surgical to replace or repair the broken bone. Some loss of function is to be expected in most patients.
References[edit | edit source]
- ↑ Free dictionary Hip fracture: Available from:https://medical-dictionary.thefreedictionary.com/hip+fracture (last accessed 14.10.2020)
- ↑ 2.0 2.1 2.2 2.3 Radiopedia NOF fractures Available from:https://radiopaedia.org/articles/femoral-neck-fracture (last accessed 14.10.2020)
- ↑ 3.0 3.1 3.2 Antapur et al. Fractures in the elderly: when is a hip replacement a necessity? Clinical Interventions in Aging. 2011
- ↑ Tinetti ME, Kumar C. The patient who falls: “It's always a trade-off. JAMA. 2010 Jan 20;303(3):258–266.
- ↑ Marks R. Vitamin C and Hip Fractures-Review. EC Orthopaedics. 2020;11:33-41.
- ↑ Bateman, Laura, et al. "Medical management in the acute hip fracture patient: a comprehensive review for the internist." The Ochsner Journal 12.2 (2012): 101-110.
- ↑ IOF Facts and stats Available from:https://www.iofbonehealth.org/facts-statistics#category-16 (last accessed 14.10.2020)
- ↑ 8.0 8.1 Zuckerman JD. Hip fracture. N Engl J Med. 1996 Jun 6;334(23):1519–1525.
- ↑ Canale ST. Campbell's Operative Orthopaedics. St. Louis, MO: Mosby;; 1998. pp. 2181–2223.
- ↑ Garden RS. The structure and function of the proximal end of the femur. J Bone Joint Surg Br. 1961 Aug;43B(3):576–589.
- ↑ 11.0 11.1 Rao, Shobha S., and Manjula Cherukuri. "Management of hip fracture: the family physician’s role." Am Fam Physician 73.12 (2006): 2195-2200.
- ↑ Dhibar DP, Gogate Y, Aggarwal S, Garg S, Bhansali A, Bhadada SK. Predictors and outcome of fragility hip fracture: A prospective study from North India. Indian journal of endocrinology and metabolism. 2019 May 1;23(3):282.Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6683687/ (last accessed 14.10.2020)
- ↑ Grisso, Jeane Ann, et al. "Risk factors for falls as a cause of hip fracture in women." New England Journal of Medicine 324.19 (1991)
- ↑ http://www.mayoclinic.com/health/hip-fracture/DS00185/DSECTION=risk-factors (visited on april 2016)
- ↑ Banks E, Reeves GK, Beral V, Balkwill A, Liu B Roddam A. Million Women Study Collaborators. Hip fracture incidence in relation to age, menopausal status, and age at menopause: prospective analysis. PLoS Med. 2009 Nov;6(11) e1000181. Epub 2009 Nov 1.
- ↑ Angthong C, Suntharapa T, Harnroongroj T. [Major risk factors for the second contralateral hip fracture in the elderly] Acta Orthop Traumatol Turc. 2009 May-Jul;43(3):193–198. Turkish.
- ↑ Yang Y, Komisar V, Shishov N, Lo B, Korall AM, Feldman F, Robinovitch SN. The Effect Of Fall Biomechanics On Risk For Hip Fracture In Older Adults: A Cohort Study Of Video‐Captured Falls In Long‐Term Care. Journal of bone and mineral research. 2020 May 13.
- ↑ 18.0 18.1 18.2 Dinçel, V. Ercan, et al. "The association of proximal femur geometry with hip fracture risk." Clinical Anatomy 21.6 (2008): 575-580.
- ↑ Handoll HH, Parker MJ. Conservative versus operative treatment for hip fractures in adults. Cochrane Database Syst Rev. 2008;(3):CD000337
- ↑ Mak JC, Cameron ID, March LM; National Health and Medical Research Council (Australia). Evidence-based guidelines for the management of hip fractures in older persons: an update. Med J Aust. 2010;192:37-41.
- ↑ Khan SK, Kalra S, Khanna A, et al. Timing of surgery for hip fractures: a systematic review of 52 published studies involving 291,413 patients. Injury. 2009;40:692-697.
- ↑ Simunovic N, Devereaux PJ, Sprague S, et al. Effect of early surgery after hip fracture on mortality and complications: systematic review and meta-analysis. CMAJ. 2010;182:1609-1616
- ↑ Moja L, Piatti A, Pecoraro V, et al. Timing matters in hip fracture surgery: patients operated within 48 hours have better outcomes. A meta-analysis and meta-regression of over 190,000 patients. PLoS One. 2012;7:e46175
- ↑ Luciani, D., et al. "The importance of rehabilitation after lower limb fractures in elderly osteoporotic patients." Aging clinical and experimental research 25.1 (2013): 113-115.
- ↑ Sylliaas, Hilde, et al. "Progressive strength training in older patients after hip fracture: a randomized controlled trial." Age and ageing (2011): afq167.
- ↑ Scheerlinck, T., et al. "Hip fracture treatment: outcome and socio-economic aspects: a one-year survey in a Belgian university hospital." Acta orthopaedica belgica 69.2 (2003): 145-156
- ↑ Daniel Pendick. ‘’After hip fracture, exercise at home boosts day-to-day function’’ Harvard health publication (2014)
- ↑ Edward Leblanc, k. i. m., and Leanne l. Leblanc. "Hip fracture: diagnosis, treatment, and secondary prevention." American family physician89.12 (2014).
- ↑ Latham, Nancy K., et al. "Effect of a home-based exercise program on functional recovery following rehabilitation after hip fracture: a randomized clinical trial." Jama 311.7 (2014): 700-708.
- ↑ Mangione KK, Craik RL, Palombaro KM, Tomlinson SS, Hofmann MT. Home-based leg-strengthening exercise improves function 1 year after hip fracture: a randomized controlled study. J Am Geriatr Soc. 2010 Oct. 58(10):1911-7.
- ↑ Wu JQ, Mao LB, Wu J. Efficacy of balance training for hip fracture patients: a meta-analysis of randomized controlled trials. Journal of orthopaedic surgery and research. 2019 Dec 1;14(1):83.
- ↑ Latham, Nancy K., et al. "Effect of a home-based exercise program on functional recovery following rehabilitation after hip fracture: a randomized clinical trial." Jama 311.7 (2014): 700-708.
- ↑ 33.0 33.1 Kannus, P., et al. "Epidemiology of hip fractures." Bone 18.1 (1996): S57-S63.

