Scapula: Difference between revisions
Joao Costa (talk | contribs) No edit summary |
Oyemi Sillo (talk | contribs) No edit summary |
||
| Line 23: | Line 23: | ||
# Lateral or Glenoid angle is broad and bears the glenoid cavity or fossa, which is directed forward, laterally and slightly upwards. | # Lateral or Glenoid angle is broad and bears the glenoid cavity or fossa, which is directed forward, laterally and slightly upwards. | ||
=== Attachments on Scapula === | === Attachments on Scapula === | ||
Scapula has various bony projections for attachment of [[Muscle|muscles]], [[ligament]]<nowiki/>s and other soft-tissue structures.<ref name="WGR">Williams GR, Shakil M, Klimkiewicz J. Anatomy of the Scapulothoracic Articulation. Clin Orthop Relat Res. Feb 1999;237-46. [Medline].</ref> | Scapula has various bony projections for attachment of [[Muscle|muscles]], [[ligament]]<nowiki/>s and other soft-tissue structures.<ref name="WGR">Williams GR, Shakil M, Klimkiewicz J. Anatomy of the Scapulothoracic Articulation. Clin Orthop Relat Res. Feb 1999;237-46. [Medline].</ref> | ||
| Line 70: | Line 68: | ||
Fung et al discovered that scapular upward rotation and retraction are greatest during abduction elevation, when compared to flexion elevation. They also discovered that posterior tilting was greatest during flexion elevation. Any disturbance in this rhythm can decrease scapulothoracic movement and can be associated with fatigue, impingement, instability, and limits in elevation. <ref name="WGR" /> <ref name="CE">Culham E, Peat M. Functional Anatomy of the Shoulder Complex. J Orthop Sports Phys Ther. Jul 1993;18(1):342-50. [Medline].</ref> | Fung et al discovered that scapular upward rotation and retraction are greatest during abduction elevation, when compared to flexion elevation. They also discovered that posterior tilting was greatest during flexion elevation. Any disturbance in this rhythm can decrease scapulothoracic movement and can be associated with fatigue, impingement, instability, and limits in elevation. <ref name="WGR" /> <ref name="CE">Culham E, Peat M. Functional Anatomy of the Shoulder Complex. J Orthop Sports Phys Ther. Jul 1993;18(1):342-50. [Medline].</ref> | ||
== Resources == | |||
Watch this 3 minute video for a recap.<ref >Scapula bone video - © Kenhub https://www.kenhub.com/en/library/anatomy/scapula</ref> | |||
{{#ev:youtube|fEXrPsGySKI|300}} | |||
== Related pathology == | == Related pathology == | ||
| Line 83: | Line 87: | ||
* [[Ewing's Sarcoma|Ewing's sarcoma]] | * [[Ewing's Sarcoma|Ewing's sarcoma]] | ||
* [[Multiple Myeloma|multiple myeloma]]<ref name=":0" /> | * [[Multiple Myeloma|multiple myeloma]]<ref name=":0" /> | ||
== References == | == References == | ||
Revision as of 21:49, 21 March 2023
Original Editor - Venus Pagare
Top Contributors - Venus Pagare, Kim Jackson, Lucinda hampton, Uchechukwu Chukwuemeka, Chrysolite Jyothi Kommu, Oyemi Sillo, Joao Costa, Naomi O'Reilly, Vanessa Rhule and Ewa Jaraczewska
Inroduction[edit | edit source]

The scapula is a thin, flat triangular-shaped bone placed on the postero-lateral aspect of the thoracic cage. It has 2 surfaces, 3 borders, 3 angles and 3 processes.
Image: Overview of the scapula bone - anterior view[1]
Osteology[edit | edit source]
The main part of the scapula, the body, consists of a somewhat triangular-shaped flat blade, with an inferiorly pointing apex, referred to as the inferior angle as well as lateral and superior angles. The scapula is described as having superior, medial, and lateral borders.
- Posteriorly, the scapula is divided into a supraspinous fossa and infraspinous fossa by the scapular spine. Anteriorly, on the costal surface, is the shallow subscapular fossa.
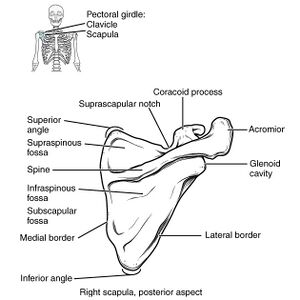
- Laterally is the glenoid fossa.
- Anteriorly is the coracoid process
- Superiorly is the acromion that is continuous with the scapular spine and arcs anteriorly over the humeral head. The suprascapular notch lies immediately medial to the base of the coracoid process. The spinoglenoid notch lies posteriorly behind the neck.[2]

Image 2: Dorsal view of the scapula

Angles
- Superior Angle is covered by trapezius
- Inferior angle is covered by the latissimus dorsi. It moves forwards round the chest, when the arm is abducted. Palpation of the inferior angle provides a convenient method for following the movement of the scapula during arm motion.
- Lateral or Glenoid angle is broad and bears the glenoid cavity or fossa, which is directed forward, laterally and slightly upwards.
Attachments on Scapula[edit | edit source]
Scapula has various bony projections for attachment of muscles, ligaments and other soft-tissue structures.[3]
Muscles[edit | edit source]

17 muscles attach to the scapula!
- Subscapularis arises from the medial 2/3rds of the subscapular fossa.
- Supraspinatus arises from medial 2/3rds of supraspinous fossa including upper surface of the spine
- Infraspinatus arises from medial 2/3rds of infraspinous fossa, including lower surface of spinthe e.
- Deltoid arises from lower border of the crest of spinthe e and from lateral border acromion.
- Latissimus Dorsi lower fibres originate from inferior angle of scapthe ula
- Trapezius is inserted into the upper border of the crest of the spine and into medial border of the acromion.
- Serratus anterior is inserted along the medial border of costal surface; 1 digitation from the superior angle to the root of spthe ine, 2 digitations to the medial border, 5 digitations to the inferior angle.
- The long head of Biceps Brachii arises from supraglenoid tubercle and the short head from the lateral part of the tip of the coracoid process.
- Coracobrachialis arises from medial part of tip ohe tf coracoids process
- Pectoralis minor is inserted into the medial borderand superior surface of coracoids process.
- The long head of triceps arises from infraglenoid tubercle
- Teres minor arises from upper 2/3rds of rough strip on the dorsal surface along the lateral border.
- Teres major arises from lower 1/3rd of rough strip on the dorsal aspect of lateral border
- Levator scapulae is inserted along the dorsal aspect of the medial border, from superior angle up to root of spinthe e
- Rhomboideus minor is inserted into medial border (dorsal aspect) opposite to root of spine
- Rhomboideus major is inserted into the medial border (dorsal aspect) between the root of spine and inferior angle
- Inferior belly of omohyoid arises from upper border near the suprascapular notch.

Ligaments[edit | edit source]
- The margin of glenoid cavity gives attachment to the capsule of shoulder joint and to the glenoid labrum
- The margin of the facet on the medial aspect of the acromion gives attachment to the capsule of the acromioclavicular joint
- The coracoacromial ligament is attached to the lateral border of the coracoids process and to the medial side of the tip of the acromion process
- The coracohumeral ligament is attached to the root of the coracoids process.
- The coracoclavicular ligament is attached to the coracoid process; the trapezoid part on the superior aspect, and the conoid part near the root. The coracoclavicular ligament is made up of 2 bands: the conoid and the trapezoid, both of which provide vertical stability. The coracoacromial ligament connects the coracoid process to the acromion.
- The suprascapular ligament bridges across the suprascapular notch and converts it into a foramen which transmits the suprascapular nerve. The suprascapular ligament lie above the ligament.
- The spinoglenoid ligayment bridges the spinoglenoid notch. The suprascapular vessels and nerve pass to it.
- The acromioclavicular ligament connects the distal end of the clavicle to the acromion and provides horizontal stability
Bursae[edit | edit source]
There are two major bursae:
- Scapulothoracic Bursa, between the serratus and the thorax, and
- Subscapularis Bursa, between the subscapularis and the serratus.
Biomechanics[edit | edit source]

The scapula upwardly rotates in the frontal plane, posteriorly tilts in the parasagittal plane, and externally rotates in the transverse plane during functional elevation. Scapular control is essential to scapulohumeral coordination. Posterior tilting is responsible for humeral clearance during the acromiohumeral portion of shoulder elevation.
Fung et al discovered that scapular upward rotation and retraction are greatest during abduction elevation, when compared to flexion elevation. They also discovered that posterior tilting was greatest during flexion elevation. Any disturbance in this rhythm can decrease scapulothoracic movement and can be associated with fatigue, impingement, instability, and limits in elevation. [3] [4]
Resources[edit | edit source]
Watch this 3 minute video for a recap.[5]
Related pathology[edit | edit source]
- Scapular Dyskinesia
- Winged scapula
- Bankart lesion
- acromioclavicular joint injury
- osteochondroma
- giant cell tumour
- chondrosarcoma
- osteosarcoma
- Ewing's sarcoma
- multiple myeloma[2]
References[edit | edit source]
- ↑ Overview of the scapula bone - anterior view image - © Kenhub https://www.kenhub.com/en/library/anatomy/scapula
- ↑ 2.0 2.1 Radiopedia Scapula Available:https://radiopaedia.org/articles/scapula (accessed 4.11.2021).
- ↑ 3.0 3.1 Williams GR, Shakil M, Klimkiewicz J. Anatomy of the Scapulothoracic Articulation. Clin Orthop Relat Res. Feb 1999;237-46. [Medline].
- ↑ Culham E, Peat M. Functional Anatomy of the Shoulder Complex. J Orthop Sports Phys Ther. Jul 1993;18(1):342-50. [Medline].
- ↑ Scapula bone video - © Kenhub https://www.kenhub.com/en/library/anatomy/scapula

